It’s a scenario many of us have experienced: You visit the dentist for a routine check-up, expecting a clean bill of dental health, only to be told you have a cavity. But wait, you think, I didn’t even feel anything! How could this be?
The truth is, cavities often don’t cause pain until they’ve progressed to a point where significant damage has been done to the tooth. This phenomenon can be attributed to the structure of our teeth and the nature of tooth decay itself.
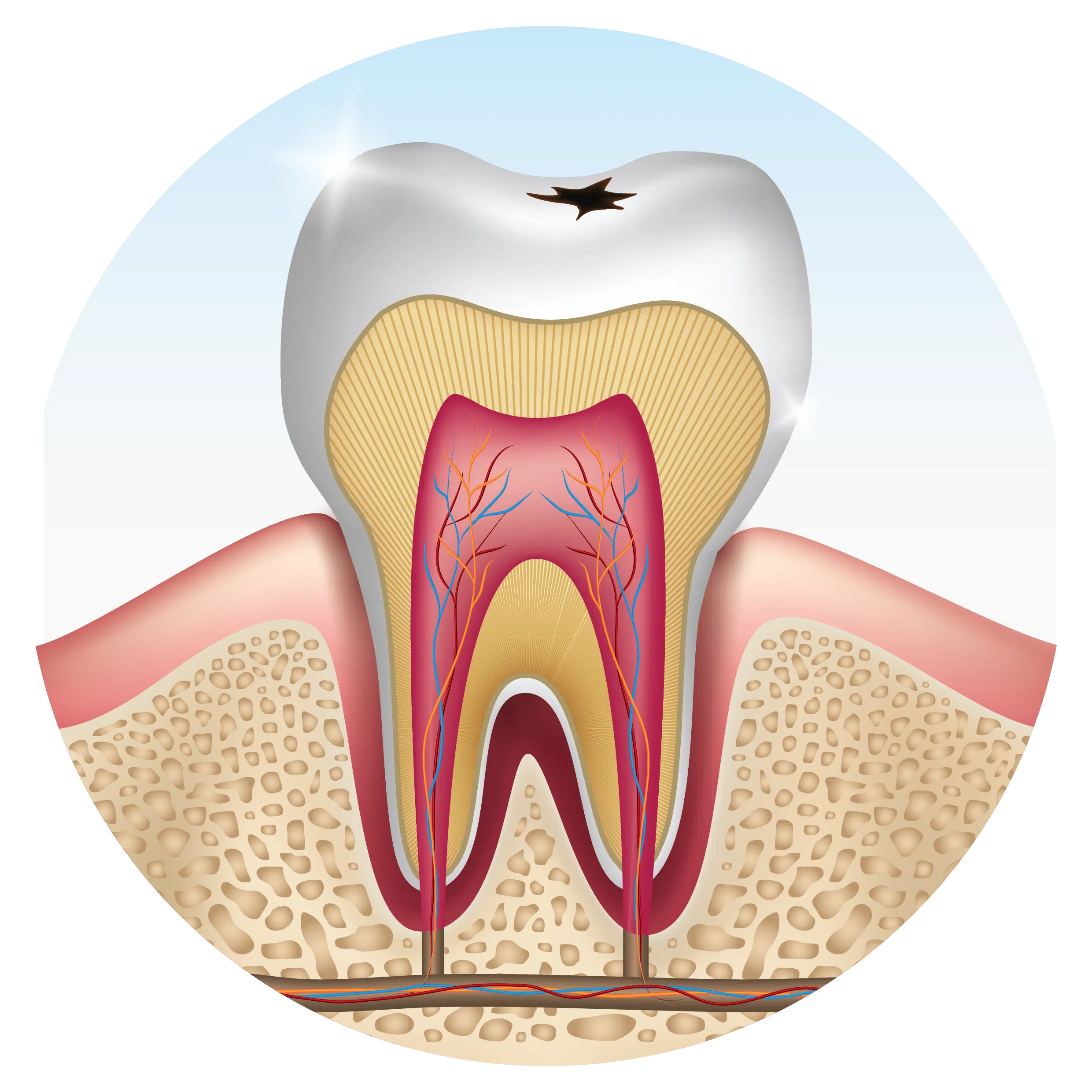
In the early stages of tooth decay, which typically begins in the enamel—the outer layer of the tooth—there is seldom any pain. This is because enamel is primarily composed of minerals and contains very few nerve endings. As a result, when decay is limited to the enamel, there are no nerves present to signal pain.
However, as decay progresses and reaches the deeper layers of the tooth, such as the dentin or pulp, where nerve endings are more abundant, pain may develop. By this point, significant damage has likely occurred, and the decay may have advanced to a stage where a root canal or extraction is necessary.
This delayed onset of pain can lead to a false sense of security for patients, who may delay seeking dental treatment until symptoms become unbearable. Unfortunately, by the time pain develops, the decay may have already caused irreversible damage to the tooth.
In many cases, dentists aim to intervene at the earliest signs of decay, typically opting for conservative treatments such as fillings, inlays, onlays, or crowns to restore the tooth’s structure and prevent further damage. These treatments are often successful in halting the progression of decay and preserving the tooth’s function.
However, there are instances where decay may be more extensive, and the decision to attempt restoration without a root canal may still be made. This decision is based on several factors, including the extent of decay, the condition of the tooth, and the patient’s overall oral health. While the goal is to preserve the natural tooth whenever possible, there are cases where restoration without a root canal may not be successful, leading to the need for additional treatment down the line.
Unfortunately, some patients may perceive the decision to attempt restoration without a root canal as inadequate care, especially if they experience pain or discomfort following the procedure. If the restoration doesn’t produce pain, this perception typically doesn’t arise in the patient’s mind. It’s important to understand that dentists carefully weigh the risks and benefits of each treatment option and make decisions based on what they believe is best for the patient’s long-term oral health.
By understanding why cavities don’t typically hurt until it’s too late and the factors involved in treatment decisions, patients can make informed choices about their dental care and work collaboratively with their dentist to achieve optimal outcomes. Prevention, early intervention, and open communication are key to maintaining a healthy smile for life.
Maybe you’re thinking: “Wow, Doc! We’re being a little dramatic here, aren’t we?” Well, read on.
No doubt, this title will elicit a few snickers and maybe even the occasional one-liner like “No, but I know someone whose breath could kill!” Nevertheless, the possibly shocking truth is that yes, bleeding gums can kill you.
As a practicing dentist, I see all levels of home care. There are patients who practice excellent hygiene and have firm, pink and healthy gums or teeth without cavities. Then there are those who probably wouldn’t recognize a toothbrush if it poked them in the eye and whose mouths have so much plaque it looks like they just finished eating cottage cheese.
The bottom line is – where along this spectrum do you fall – and what can it mean for your overall health?
As I write this, I recall a question posed to me by one of my patients just yesterday. He told me that one of his “lady friends” had recently passed away. According to his story, he had seen her a few weeks ago and then noticed she wasn’t around very much. When he asked about her, he learned she had died as a result of complications following a dental abscess. His question “is that possible?” reflected an incredulity that is typical when it comes to the effects of oral health on the body.
Again, my answer was “yes, it’s possible.” Severe sepsis, which is basically a systemic inflammatory response to infection, can lead to organ failure and death. His friend was forty-two years old.
Obviously, this is an extreme example of infection travelling from one site and affecting the entire organism, but there are more subtle examples that are no less significant. Take bleeding gums. There are probably few people who haven’t experienced this phenomenon at some point or another in their lifetimes. If you are a hypochondriac, you probably should stop reading right now. If, on the other hand, you are just interested in knowing what significant step you can take to reduce your risk for heart attack or stroke, read on.
If I were to speculate, I think that many physicians and dentists probably still don’t think of tooth-related infections as systemic risk factors. The science behind this concept, however, is clear. In fact, a number of studies have been completed which clearly show the following:
Tooth-related infection can cause death
Infection equates to heart attack and stroke
Periodontal diseases are a portal for systemic inflammation and disease
If you have a periodontal infection you are going to have elevated C-reactive proteins, and C-reactive proteins are four times more predictive of cardiovascular complications than cholesterol
References for these studies will be made available on my website. But that represents a relatively small sampling of the articles which conclude red gums represent a disease process unto itself. This observation is the critical point.
If red gums represent inflammation and infection, then bleeding gums are definitely not something you should ignore. Even if you are not worried about your health, you may be surprised to know that many clinicians believe that aging is caused by systemic inflammation. There are a few studies supporting this theory as well, but the point is simple: don’t ignore your oral health. You might even look younger if you take care of your teeth! One of the simplest ways to reduce inflammation is to control the bacteria in your mouth. Start by brushing after meals and flossing every day. Eat a proper diet rich in vitamins and minerals. Get enough rest. Exercise, and reduce stress.
Also, don’t forget to visit your dentist regularly. Because so many dental conditions are symptom-free in their early stages, patients can be hit hard by neglect. The perception of “no pain, no problems” is often misleading when it comes to dental problems. Couple this with the fact that in tough economic times, people tend to put off what they perceive as optional or unpleasant, and you can have a formula for disaster – financial, or otherwise….
Many people believe that since they aren’t experiencing dental symptoms – like tooth pain or bleeding gums – then all must be well.
Unfortunately, a sizable number of dental problems, including cavities and periodontal disease (bone loss around your teeth), just don’t produce obvious symptoms in their early stages. At least not symptoms that tend to be obvious to patients.
In fact, by the time people the average person experiences pain, his dental issue is typically pretty far along. And all too often, by then, the problem can also be quite expensive to handle.
It might amaze you to discover the types of problems your average dentist encounters every week, many of which you would expect to be painful, but they just aren’t. They can still result in tooth loss though.
Pretty much anyone who has ever worked in a dental office for any length of time will tell you this is so. And they will tell you that you can inform some people that they have a problem, but unless it is “real” to them, they just won’t do anything about it.
They may come back a few years later (or maybe sooner) – usually with an emergency – desperately wanting to save the tooth that you told them about earlier. Of course, by now, it may be too late. And very often they will have forgotten it was ever discussed at all, because it was never a realistic problem for them to begin with.
Human nature can be funny that way.
So, keeping that in mind, it’s generally a good idea to get checked out by a dentist. Regularly.
The best news you can hear is that everything looks great.
But sometimes getting a confirmation that you don’t have cavities or gum disease is not the only reason to get a dental exam. Over the years, I have detected cancer (not just oral cancer) – as well as a host of other non-dental problems – that might have been overlooked had the patient not scheduled an exam. Obviously, we refer patients to an appropriate specialist for treatment when we discover medical problems outside the scope of dental practice.
Other benefits of getting a dental exam: I can recall many patients who told me that what they thought were unrelated health problems simply resolved when their oral problems were gotten under control. These have included digestive problems, low energy problems, elevated blood cell counts, hypertension, and more.
Over the years, some people have told me they don’t want to get a dental exam because they don’t want to discover they have any problems. I guess that works.
Just maybe not too well.
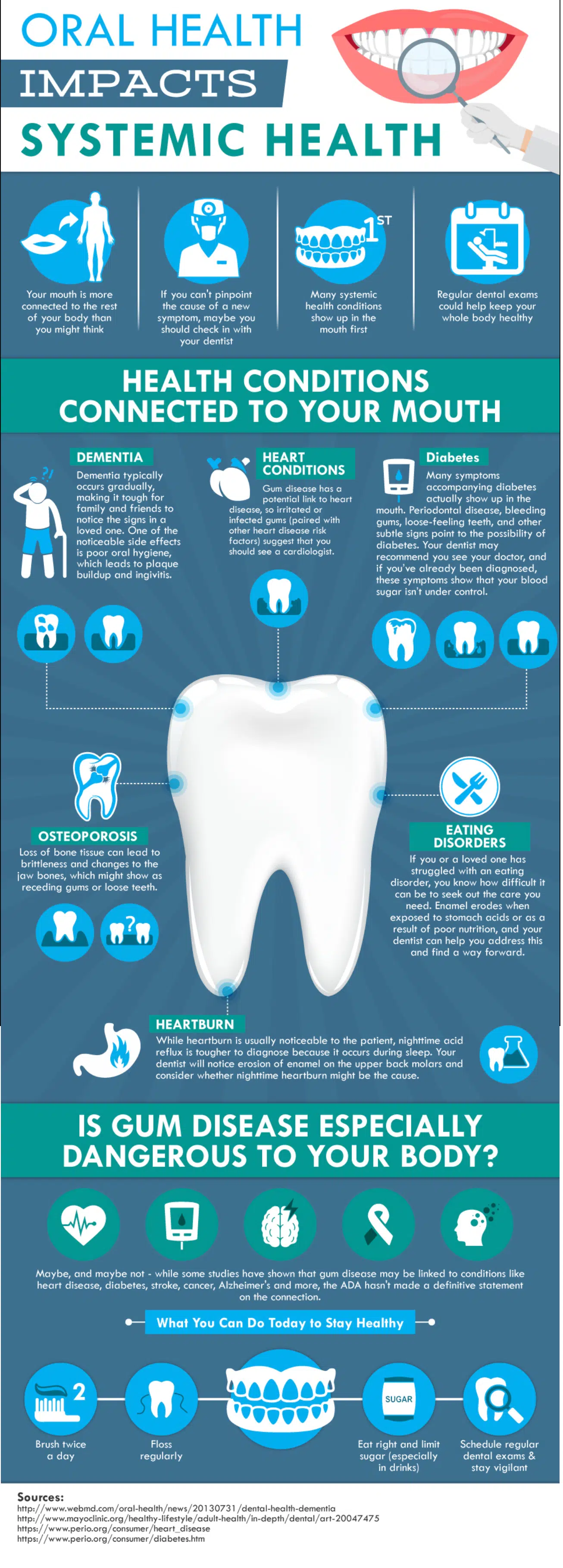
Your overall health is connected to your oral health. Take a look at this infographic. Then think it over. . . .
Because tooth-loss so often creates long-lasting and generally negative effects for personal health and, not infrequently, appearance – the entire array of tooth replacement options has long been an important subject in the dental field. Dentists not infrequently discuss which options are best for their patients, given different circumstances. And if there is any debate in the profession at all, you can be sure the public will also question which options make the most sense for them.
The truth is there is no one right answer. Each person’s circumstances differ – whether the reasons are anatomic, functional, emotional, or financial.
But the question is still an important one to ask, because patients face new realities when they lose even one tooth. These changes include (but are not limited to):
Difficulty chewing
Altered speech
Food impaction
Jaw pain
Drifting teeth
And, then there are the secondary effects:
Poor health resulting from a changing diet
Compromised appearance
Self-consciousness/embarrassment
An inability to wear dentures
Financial challenges created by the need to address these problems
It is this last point that I want to touch upon here, because I have observed a good deal of confusion surrounding dental implants. As a dentist, I am obligated to review all options with an individual when discussing their tooth replacement options – regardless of affordability. I can’t, and don’t, pre-judge anyone financially when discussing their choices.
Commonly, though, when I raise the subject of dental implants, I get an immediate reaction along the lines: “Oh, forget it. I could never afford that. How about a bridge?”
Now, I’m not going to try to convince you that implants are cheap. Restore a full mouth with dental implants and it is likely to be costly. Nevertheless, cheap is relative. For some of my patients, even a small filling can be perceived as expensive. For my wealthy patients, they might be prepared to spend any price for what they perceive will serve them best. Lucky them. Right?
What I hope to do here, however, is to show you when an implant may make the most sense for a person. And — at least, when when it comes to replacing a single tooth — a dental implant may just be the way to go.
But first, permit me to remind you again – there is no one right answer for everybody. Your choices may be very different depending upon whether you are 25 or 85 years old, for example.
I’m sure you can fill-in still other reasons that affect your decision-making process. But for now, let’s consider the following scenario:
A patient loses one tooth.
For the sake of argument, we’ll call it a lower right first molar. Suddenly, the patient realizes this is annoying. Their bite is changing; their gums are sore. They feel the need to do something. Now.
Here are a few options. I’m just going to list the main ones, but there are sub-sets to some of these:
Do nothing anyway.
A removable denture.
A non-removable bridge,
A dental implant.
For the purposes of this discussion, the patient has already decided that doing nothing isn’t working for them.
So, the next option is a removable denture. I usually get “the face” on this one.
And with good reason. Food gets caught around partial dentures every time you eat. You will have to remove the appliance after EVERY meal and clean it separately from your own teeth. Certain foods will also cause it to dislodge as you eat, allowing some of the food to get caught between the denture and your gums. The cost – depending upon what kind of partial you have made – will typically range between $750 and $1,500.† The recommended replacement time: every 5 to 7 years. The reality – people replace them roughly every 15 years. Sometimes more. The longer they put off the replacement though, the more issues they may face with the replacement.
Bottom line: Removable dentures are potentially uncomfortable. Average lifetime replacement cost if you are 25 years old, (based on an average life expectancy of about 79 years, and an average 10-year replacement rate – not adjusting for inflation) is going to be nearly $7,000.
Next, we’ll take up considering a “bridge.” It’s called a bridge because it spans a gap (like a bridge spans a body of water) with a fake tooth, or teeth, in between the ones that are still there. The trouble is that you must shave down the supporting teeth to little stubs so that the result will look natural and be strong enough to take the force of daily chewing. For the most part, bridges look, and can often feel like, your natural teeth; but you do have to floss under the fake tooth after every meal. Food will get caught under there, whether you perceive it or not. If you don’t clean it regularly, the life expectancy of your bridge will be shorter.
Now, the cost on this option can really be widely variable, because some teeth need to have fillings replaced before they can be used as supports for the bridge. In other cases, the teeth may end up with root canals if the process of shaving them down results in lingering sensitivity. This doesn’t always happen, but it is a risk. If the tooth needs that additional treatment it will cost you more.
The average cost to replace a single tooth with a bridge is about $3,500. Again, that can be a little more, or less, depending upon what part of the country – or even what part of a city, you live in.
If, on the other hand, you also need to place or replace fillings on the teeth being used as supports, and you need to do root canals as well, it could be as much as $7,000.
Roughly, double.
The average lifetime replacement cost with the same parameters given above (25 years old with an average life expectancy of 79 years and a 10-year average replacement rate) is going to be: $31,500. And that assumes that the underlying teeth will be strong enough to survive that many replacements.
That brings us to dental implants.
Here is the breakdown: The average implant cost in many metropolitan areas is around $1,800 – $2,200. If you end up needing a bone graft before the implant can be placed, though, add another $550. (Basically, a graft is adding bone to your jaw when you don’t have enough for the implant.) So far, these costs are just for the implant. It doesn’t include the cost of the crown. Add about another $2,100 for the parts needed to make up what supports the crown above the gumline, and the crown itself. If your tooth is short, and there isn’t enough tooth height to which your crown can be easily cemented, you might need something called a UCLA abutment — it lets your dentist screw down the crown instead of cementing it. That could cost you more. How much depends upon the lab your dentist uses, but $500 more wouldn’t be unusual.
On the low end, one implant may cost $3,900. On the high end, let’s round up to $4,900.
So, what about the average lifetime cost?
$4,400.
That’s less than either partial dentures or bridges!
Why?
Because, unless you bite into a rock, grind your teeth uncontrollably, or have some serious illness that causes you to lose bone around the implant – any of which can happen to you with the other options as well – you will probably have your implant for life. Still, no one can guarantee this because, sometimes, plain ol’ dumb luck will factor into any equation.
But, you can’t get a cavity on an implant. On the other hand, you still can get a cavity on the teeth that support your partial denture, or bridge (and crowns, for that matter).
So, do the math. Look at your circumstances, and decide what is right for you. But when your dentist starts talking to you about dental implants, hear them out. It just might be more cost effective than you realize.
† [Note: The prices mentioned here are just averages in US Dollars at the time of this writing. Actual costs could be more, or less, depending upon where you live.]
First of all, what the heck is vitamin P? First discovered around 1936, the term is hardly used anymore – except maybe euphemistically for Prozac (fluoxetine) – which you definitely don’t need, unless you like playing Russian roulette with your health. Prozac is widely regarded as one of the most dangerous drugs on the market. More about that some other time, perhaps.
But, real Vitamin P is better known today as a plant classification called flavonoids or bioflavonoids.
[Because of my interest in natural health, I subscribe to a number of health-related newsletters. One of them (and I recommend this newsletter to anyone interested in sensible health and nutrition) recently reminded me of a subject I have already written about on a number of occasions. Namely, the importance of controlling inflammation, actions one can take to do so, and the nutrients that can assist with this problem. The newsletter I’m referencing here is called Health Alert, by Dr. Bruce West. Much of what follows in this posting comes from that source. If you are interested in subscribing, their number is 831-372-2103. I receive no financial benefit by recommending them. It’s just good information.]
Nevertheless, here’s why real vitamin P is important to your health, and yes, even more specifically – to your dental health:
The cells that line your blood vessels are truly amazing in terms of all the functions they provide. Their end-result have a great deal to do with how you heal. But they can’t do their job without the adequate nutrition that they need. And the prime nutrient required by these cells is vitamin P. Originally, vitamin P was named for an extract of paprika. Today, we know it better as bioflavonoids.
But if you are deficient in vitamin P, you are likely suffering from sub-clinical scurvy.
At one time, scurvy was considered deadly. Today, it is looked upon as an old disease that has been pretty much eradicated. But the less deadly version – sub-clinical scurvy – can be found in much of the American population. It’s even possible you may have it.
And while you probably won’t die quickly from scurvy as people did centuries ago, your odds of dying from damage to your blood vessels and the resulting strokes and/or heart attacks are significantly increased. If you notice your toothbrush looks a little pink when you brush, or if you have outright bleeding gums, or possibly blood stains on your skin as a result of leaking blood (Schamberg disease), or you have been diagnosed with coronary artery disease, blood clots, plaque, stroke, heart attack, deep vein thrombosis, peripheral artery disease, and most other circulatory problems – you are suffering from sub-clinical scurvy and you need vitamin P.
Vitamin P feeds the lining cells of your blood vessels – called endothelial cells – and can restore your health after they have been suffering from a vitamin P deficiency. That makes vitamin P a natural anti-stroke, anti-clot, and anti-heart attack nutrient. It will help regenerate your endothelial cells to heal your blood vessels properly. It will even help to keep your blood flowing better (by making them less stick and sludgy) without the many side effects of poisonous blood thinners.
As a dentist, I know that vitamin P is also helpful in your fight against gum disease and tooth loss. More teeth are lost (worldwide) due to periodontal disease (bone loss around the teeth) than to any other factor. Vitamin P deficiency has a lot to do with this. But it doesn’t end there. Because of its direct effects on collagen, vitamin P can also help you with ulcerative colitis, frostbite, arthritis, varicose veins, hemorrhoids, and more. It is even protective against radiation damage.
But, by far, its main benefit is to the linings of your blood vessels. And when it comes to your gums that’s crucial.
All kinds of products claim to be able to heal your blood vessels. Frankly, most of them don’t work. If you truly want to heal your blood vessels, then the most effective source of vitamin P, by far, is the juice of deep green buckwheat leaves harvested at the time of their peak nutritional content. Possibly, the most powerful bioflavonoid in buckwheat juice is called rutin. Now, most of us aren’t going to start an organic garden to grow buckwheat — that we then harvest at the optimal time — and then make juice from the leaves. And, fortunately, we don’t have to.
One company – Standard Process – does that all for us. They make the supplement Cyruta-Plus in a tablet that contains all the life force, nutrients, and bioflavonoids of the juice itself. If you have gum problems, or any of the other problems listed above, 2-4 tablets of Cyruta-Plus 3x daily, would be a good place to start. Give it one to two months to help repair the damage already caused by what has probably been a long-term deficiency.
If you are not easily convinced and need additional proof (other than observing the results for yourself), you can ask your doctor to have your CRP (C-reactive protein) level checked. Most people with blood vessel inflammation will have an elevated CRP in their blood. If this is you, this is an inflammation marker, and your chance of having a heart attack or stroke becomes significantly higher.
You might be tempted to try one of the advertised “super-potent, artery scrubbing” anti-oxidants which are advertised, like reservatrol or ascorbic acid. Go ahead and try it. Then have your doctor order a new CRP blood test. After that treatment fails, try Cyruta-Plus (9 – 12 daily for 30 days) and get one more blood test. See what happens. Chances are you will be both shocked, and happy.
Not only will you have helped your gums and teeth, but you will have lowered your risk of heart attack and stroke, you will have helped your joints by improving arthritis, your gut will enjoy better digestion, your skin will thank you, as will your legs. Plus, the potential for living longer is not a bad result either.
Dr. Richard Walicki is a dentist practicing general and cosmetic dentistry. While we hope you find the information contained herein interesting and useful, this blog is for informational purposes and is not intended to diagnose any oral disease. Dental conditions should be evaluated by your dental health professional or a qualified specialist.
Search by Topic
Get Access To The AWESOME Health Course
In this 12 week program, you’re going to discover how to achieve AWESOME health and double your energy with natural, tested, and scientific strategies. Just click on the image below: