More people are keeping their natural teeth for life, which is good news for smiles—but it also means we are seeing more teeth develop structural problems over time. Heavy biting forces, large fillings, root canal treatments, and day-to-day stress can all weaken a tooth and set the stage for what dentists call a cracked tooth. In fact, cracked tooth problems are now one of the more common reasons adults report mystery biting pain.
If you are interested in a more technical background, you can also read my earlier article here: Cracked Tooth Information. The article you are reading now is designed as an updated, easy-to-follow guide to help you recognize the signs and understand your options.
Why are cracked tooth problems becoming more common?
Several trends are driving the increase in cracked tooth issues:
We live longer and keep our teeth longer. Older teeth have been through decades of chewing, temperature changes, and dental work. Large fillings and endodontic treatments remove tooth structure and can leave the remaining tooth more fragile, making a cracked tooth more likely over time.
Stress, clenching, and grinding are on the rise. Many people clench or grind their teeth when they are focused, anxious, or asleep. Some medications, including certain antidepressants (SSRIs), are associated with increased bruxism, which can amplify these forces and increase the risk of a cracked tooth.
Substance use can accelerate damage. In patients with a history of methamphetamine or other stimulant use, severe bruxism and dry mouth often combine to produce shortened, worn, and cracked teeth.
Dentists are simply better at finding cracks. With improved lighting, magnification, and imaging, cracks that once went unnoticed are now diagnosed more often.
Typical cracked tooth symptoms
Cracks do not always behave like a “normal” cavity or toothache. When you have a cracked tooth, the symptoms can seem a bit strange or inconsistent.
Sharp, brief pain when chewing or biting. Pain often occurs as you bite down or when you release biting pressure.
Sensitivity to temperature, especially cold. A sip of cold water or air can trigger a quick, sharp twinge.
Pain that comes and goes. You may go days feeling fine and then suddenly get a streak of discomfort when you chew on a certain area.
Normal tap test. Tapping with a dental instrument (percussion) may not reproduce the pain, which can make the problem more confusing.
Important: These symptoms are not proof of a cracked tooth. Other conditions, such as inflamed pulp or gum problems around a tooth, can feel very similar. A proper diagnosis always requires a clinical exam.
Why a cracked tooth can be hard to diagnose
From the dentist’s side, crack-related problems can be some of the most challenging cases in everyday practice. Cracked tooth syndrome is known for variable, sometimes vague symptoms and for being difficult to confirm on X-rays.
The “mystery tooth” story
Many patients describe a long history of odd biting pain that is hard to put into words. They may have:
Episodes of sharp pain when chewing on one side, but not every time.
Cold sensitivity that comes and goes.
No obvious pain when the tooth is tapped or pressed.
Dental X-rays that look normal, or nearly normal.
It is not unusual for someone to see more than one dentist, try different adjustments or restorations, and still have symptoms before a cracked tooth is finally identified. In some cases, a 3-D scan (CBCT), transillumination, or special dyes are needed to make the crack visible. Other times, the true extent of the problem is only discovered after an old filling or crown is removed, or when a narrow, deep periodontal pocket appears along the root.
If you would like to see how a professional organization describes this condition, the American Association of Endodontists has a helpful page on cracked teeth here: Cracked Teeth – AAE.
How serious can a crack become?
Not all cracks are equal. Tiny craze lines in the enamel are extremely common and are usually harmless. Deeper cracks that extend into the dentin, or all the way into the pulp, are more concerning:
Shallow structural cracks may cause biting sensitivity but can often be stabilized with an onlay or crown.
Cracks that reach the pulp can inflame or infect the nerve inside the tooth, leading to lingering pain, swelling, or an abscess if bacteria enter.
Vertical root fractures that extend down the root often have a poor long-term prognosis and may require extraction.
The earlier a significant crack is diagnosed, the more options you usually have to protect and preserve the tooth and avoid losing it altogether.
What you can do if you suspect a cracked tooth
If you notice biting pain, temperature sensitivity, or a pattern of “mystery” tooth discomfort that comes and goes, it is worth getting it checked promptly. Here are practical steps you can take if you suspect a cracked tooth:
Pay attention to patterns. Gently test chewing on one side and then the other. Note whether the pain occurs on biting, on release, or with cold drinks, and share this with your dentist.
See a dentist sooner rather than later. Waiting for the pain to “settle down” can allow the crack to deepen, sometimes turning a restorable tooth into one that needs extraction.
Ask what the exam will include. In addition to regular X-rays, your dentist may use magnification, fiber-optic light, special bite tests, or 3-D imaging to look for subtle cracks.
Discuss all reasonable treatment paths. Depending on the crack’s location and depth, options might range from monitoring and protective bite guards to restorations, or in some cases, referral to an endodontist for further evaluation.
About root canal treatment: When a crack has irritated or infected the pulp, many dentists will recommend root canal therapy as a way to keep the tooth rather than remove it. Whether that makes sense for you depends on the extent of the crack, how the tooth fits into your overall health priorities, and how you feel about this procedure. A thoughtful, individualized discussion with your dentist or endodontist is essential before deciding.
Reducing your risk of future cracks
You cannot control every variable, but you can lower your lifetime risk of a significant cracked tooth with a few practical habits:
Protect your teeth from excess forces. If you clench or grind, especially at night, ask about a custom nightguard. Address high-stress habits like chewing ice, pens, or very hard foods. The American Dental Association also has a useful overview of bruxism and nightguards here: Bruxism – MouthHealthy.
Maintain and update older dental work. Very large or aging fillings may need to be replaced with stronger restorations before they fail. Regular checkups make it easier to catch these issues early.
Support your enamel and overall oral health. A diet that minimizes frequent sugar and acid exposure, along with good daily home care and appropriate professional products, keeps the outer shell of the tooth more resilient. For a deeper dive into enamel repair and protection, see my article on enamel remineralization.
Think whole-body, not just tooth-by-tooth. Systemic health, medications, sleep quality, and nutrition all influence how your teeth handle stress over time. If you are interested in nutritional and supplemental support for oral and general health, you can learn more on the ToothWiz Vitamins page.
When to seek urgent care
Most cracked tooth problems evolve gradually, but some situations deserve same-day attention:
Sudden, severe pain after biting on something hard.
A piece of tooth or filling that breaks off.
Facial swelling, pimple-like bumps on the gum, or throbbing pain that keeps you up at night.
If any of these occur, treat it as a dental emergency and contact a dentist or urgent care provider as soon as possible.
Bottom line: listen to your teeth
Cracks are not always easy to see or simple to diagnose, and the symptoms can be confusing—even for experienced clinicians. But they are also very real, and catching a cracked tooth early can mean the difference between a conservative restoration and losing the tooth.
If you have unexplained biting pain or temperature sensitivity that just does not feel right, trust your instincts. Get it evaluated, ask questions, and take the time to understand your options so you can choose the path that fits both your mouth and your values.
Many people believe that since they aren’t experiencing dental symptoms – like tooth pain or bleeding gums – then all must be well.
Unfortunately, a sizable number of dental problems, including cavities and periodontal disease (bone loss around your teeth), just don’t produce obvious symptoms in their early stages. At least not symptoms that tend to be obvious to patients.
In fact, by the time people the average person experiences pain, his dental issue is typically pretty far along. And all too often, by then, the problem can also be quite expensive to handle.
It might amaze you to discover the types of problems your average dentist encounters every week, many of which you would expect to be painful, but they just aren’t. They can still result in tooth loss though.
Pretty much anyone who has ever worked in a dental office for any length of time will tell you this is so. And they will tell you that you can inform some people that they have a problem, but unless it is “real” to them, they just won’t do anything about it.
They may come back a few years later (or maybe sooner) – usually with an emergency – desperately wanting to save the tooth that you told them about earlier. Of course, by now, it may be too late. And very often they will have forgotten it was ever discussed at all, because it was never a realistic problem for them to begin with.
Human nature can be funny that way.
So, keeping that in mind, it’s generally a good idea to get checked out by a dentist. Regularly.
The best news you can hear is that everything looks great.
But sometimes getting a confirmation that you don’t have cavities or gum disease is not the only reason to get a dental exam. Over the years, I have detected cancer (not just oral cancer) – as well as a host of other non-dental problems – that might have been overlooked had the patient not scheduled an exam. Obviously, we refer patients to an appropriate specialist for treatment when we discover medical problems outside the scope of dental practice.
Other benefits of getting a dental exam: I can recall many patients who told me that what they thought were unrelated health problems simply resolved when their oral problems were gotten under control. These have included digestive problems, low energy problems, elevated blood cell counts, hypertension, and more.
Over the years, some people have told me they don’t want to get a dental exam because they don’t want to discover they have any problems. I guess that works.
Just maybe not too well.
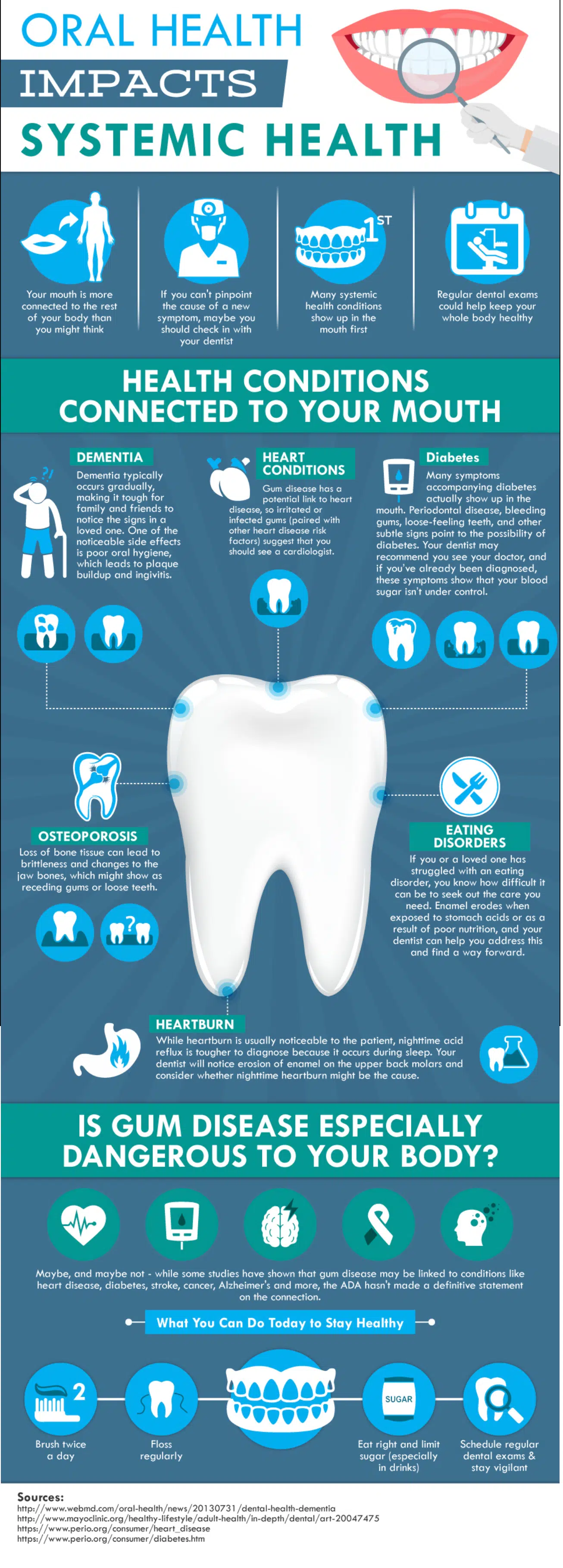
Your overall health is connected to your oral health. Take a look at this infographic. Then think it over. . . .
I have little doubt that some patients who visit a dentist and are told they have decay, but don’t experience any symptoms, are convinced that someone is trying to pull the wool over their eyes. There are probably several reasons for this. Possibly, they had been to some unscrupulous person in the past who suggested they had a problem, when they really didn’t.
I can see how that might create skepticism. I mean, it’s conceivable that sort of thing could happen.
But even if that were the case, I sincerely don’t believe it represents the behavior of a majority of dentists. Most of the dentists I know genuinely care about what they do and the people they treat. So maybe these skeptics are just people who don’t trust anyone. I don’t know.
The reality, though, is that these patients will eventually be in for a big surprise when the you-know-what hits the fan. Or – and let’s keep this a family column — when the decay hits the nerve.
But that could take a while.
And I believe that could be where some of the problem lies. A patient tries to use this to their advantage — they want to buy some time. After all, it’s not really being a “problem” for them in that they don’t perceive anything as being different. When the problem eventually does occur, I usually hear: “I never thought it would happen to me.”
A doctor detecting treatable decay usually recommends that the patient handle it at their earliest opportunity.
Why? Well, the patient can catch the problem when it is small, when it is less likely to cause post-operative discomfort, and when it will generally cost them a lot less.
But, first, let’s back up a little and explain why it’s possible to have a cavity – several in fact – and have absolutely no symptoms.
Most decay starts on the outer surface of the tooth called the enamel. It’s roughly 97% mineral in consistency and does not contain nerves. That means it has no feeling. Practically zero. Your dentist could DRILL on that part of the tooth and most of the time you won’t feel it.
Notice that in the earlier paragraph I mentioned “treatable” decay. Well, when would decay not be treatable right away? I can’t speak for other dentists, but I typically won’t treat decay when it is confined to the enamel. Why? It has the potential to re-mineralize. In other words, it has the capacity to fix itself – that is, if you don’t continue to do the things that led to the cavity in the first place. Usually, this is related to your diet, but it can be affected by hormones, or even medications.
Why not mention home care first? Isn’t that important too? Of course it is. It just may not be the most important factor.
Another time a dentist might not treat a cavity could relate to the age of the patient. For a much older patient, there are times when the pain or infection are not likely to come up before the patient passes. Of course, your dentist doesn’t have a crystal ball on that point. (Well, probably not.) But, it wouldn’t make sense to recommend treatment in the majority of those cases.
And this takes us back to the nature of a cavity. They often take a long time to get bigger. (But not always…. Again, no crystal ball here.) The reason has to do with the hardness of the enamel itself. Enamel, for you trivia lovers, is the hardest substance in your body. It’s harder than bone, and that property, along with the lack of sensation, can be problematic.
Here’s why: a cavity is often quite small on the outside of the tooth. It’s actually difficult for decay to work its way through that hard enamel. Most of the time it burrows a narrow channel down to the dentin (only a couple of millimeters away) and then it really starts to spread. Because dentin is softer than enamel, it’s just easier for it to spread more quickly there. By the way, this additional, and deeper, decay – very often still doesn’t hurt – as long as it is far enough away from the nerve.
Meanwhile, your enamel is, for the most part, continuing to hold its form. That stuff is hard. But things are generally hollowing out on the inside of the tooth now — out of sight and out of mind — as the decay continues to spread. Painlessly.
Eventually, your tooth can become very much like an eggshell.
Then one fine day you bite on something, and the hard enamel that was still doing its job holding the form of the tooth caves into the hole below. It just got too thin.
Now, at this point, does the skeptic understand that he got a cavity? Sure. Some of them finally get it. But for others –no! It’s more like: “Hey that blowhard dentist was obviously wrong because he talked about me having cavities years ago, and look – I did fine until now. In fact, I probably just lost a filling! Jeez, this hole just came out of nowhere. It’s probably the fault of some earlier dentist.” (Um, Mr. Skeptic never got the filling though. Remember?)
“Hey doc, how much is this going to cost me? $2,400?!!! (For a root canal, buildup and crown.) Are you insane? Just pull it.”
Now you are going to be missing a tooth, and may lose even more teeth as a result. Yet, when the doc first mentioned it, that cavity was only going to cost $150. How can it suddenly become sixteen times more expensive?!
“Rip-off artist. Seems you can’t trust anyone. . . .”
No matter how you slice it, tooth problems can be a pain. Among these, cracked teeth stand out for their confusing and erratic nature. A cracked tooth can be painful, annoying, and an exercise in frustration for patients and dentists alike. While there can be many factors that contribute to cracked teeth, the bottom line is that if your tooth is cracked the solution is often involved, potentially expensive — and, despite best efforts, tooth loss is still a very real possibility. Clicking on the picture below will take you to a compilation of questions and answers about cracked teeth. It covers a lot of ground, but if you think you may have a cracked tooth, it is worth reading so that you can know what to expect.
Consider this article a public service announcement. I really dislike it when patients lose their teeth unnecessarily. My practice philosophy is that if a person has a dental problem, the goal is to handle that difficulty first, but then empower the patient with the correct knowledge that will keep him out of trouble from there on out. Ideally, my hope is that most future visits to my office will only be for routine maintenance.
Unfortunately, and all too often, I encounter new patients with teeth that are so badly decayed there is little hope of salvage. Possibly just as frequently, I find these patients scheduling a checkup – usually after a long absence from dental care – who are surprised to learn that they have any cavities at all. Sometimes they will think they lost a filling when, in fact, a piece of their enamel has broken away.
Why are they surprised? The common denominator seems to be the idea that cavities are supposed to hurt.
Well, sometimes they do hurt. But most of the time – especially in the early stage – they don’t.
In fact, by the time a tooth does start to hurt you it’s usually pretty bad. More often than not, it is so bad that a dentist is evaluating whether it can be treated with endodontic (root canal) therapy or whether it needs to be extracted. A little understanding of basic dental anatomy is helpful here.
Take a look at the illustration below:
The outer layer of the tooth is comprised of enamel. This is the hardest substance in your body. It breaks up your food and is designed to last you a lifetime.
And now, here is the important part for you to understand: it doesn’t contain any nerves.
It is more than ninety-five percent mineral. Water and organic materials make up the balance. And because it doesn’t have nerves, it doesn’t have feeling. This is actually quite practical since it wouldn’t do to have pain every time you bit into something. On the other hand, it also means that it can be decayed without giving you a warning.
In fact, decay can also travel into the supporting layer – the dentin – and still not cause you pain. It usually has to travel pretty close to the inner layer that contains the blood vessels and nerves – the pulp – before you feel it. Of course, by then, the tooth has generally undergone considerable destruction.
Another factor that makes spotting decay difficult is the way it spreads. I have drawn two black triangles into the enamel above. Notice that the narrow point is on the outside of the enamel. The broader base faces the inside of the tooth. This is how decay usually travels. Sometimes, it will undermine the interior of the tooth while the outer, harder enamel still maintains its form . . . until it eventually crumbles because the underlying supporting dentin has been eaten away by decay.
Many cavities also form at the contact point between two teeth. These are areas that you simply cannot see. Even the dentist needs an x-ray to spot these cavities in most cases.
So what does all this really mean? Spotting decay is not always that easy. As dentists, we use visual examination, but we also rely on probes, x-rays, and even laser detection devices to locate cavities. Even then, it can be difficult to find cavities under existing fillings.
Don’t rely on pain to tell you if you have a cavity in your tooth. If you do, you can be assured that your treatment is likely to be more uncomfortable, expensive, and may even result in the loss of a tooth that could have been treated much more easily earlier in the game.
If you have a loved one, who still has their teeth and hasn’t seen a dentist in a while, have them read this article. You may be saving them from quite a bit of discomfort – not to mention time and money – if they catch potential problems before they are hopeless.
Some of you may be thinking, “No big deal. If it’s that bad, I’ll just pull it.” OK, sometimes that is necessary, but therein lies a lesson for another day.
My guess is that it is either because you are compelled to do so by law, or (if you live in the U.S.) you believe the National Highway Traffic Safety Administration (NHTSA), who claim that seat belts save about 13,000 lives a year, nationwide.
The few seconds it takes you to snap on your seat belt buckle reduces the chance of dying in a car crash by 45%, and of being injured by about half. Nevertheless, seat belts are not likely to play a big role in saving your life, because chances are you won’t find yourself in a serious automobile accident. Let’s face it, fortunately, most people never find themselves in that circumstance.
On the other hand, gum disease (either gingivitis or periodontal disease) affects up to 80 percent of the population.
In other articles, you may have heard that periodontal disease is the leading cause of tooth loss among adults. The shocking reality is that this is probably the least notable consequence of periodontal disease.
Periodontal disease is a significant risk factor for stroke, heart disease, certain respiratory problems, low birth-weight infants, and some forms of cancer.
While very few people will die in a car crash, a great deal more will die from a heart attack, stroke, or cancer. Addressing periodontal disease via preventive techniques can significantly reduce your chances of dying from any one of these afflictions.
If this simple logic is not enough to convince you of the need to brush after meals, floss daily and eat a healthy diet, it may help you to know that over the past few decades, there have been hundreds of peer-reviewed medical studies published in journals showing periodontal disease to be a risk factor for heart attacks.
While periodontal disease is certainly not the only factor in the occurrence of cardiovascular diseases or cancer, there is definitely a link. The modern thinking regarding the connection has to do with the long-term inflammatory nature of gum disease. In simple terms, periodontal disease is a bacterial infection of the gums and bone supporting the teeth. As with most any infection in the body, this leads to inflammation.
Often having no symptoms that are detectable by the patient, bacteria from periodontal disease can affect blood vessels on the walls of your heart. If you have gum disease, the bacteria can easily invade the blood stream through one of many open portals. Let’s face it, it is a relatively short trip from the mouth to the heart after all.
Bacteria in the blood may also stimulate liver production of C-reactive proteins and fibrinogen. Both these substances have been linked to heart attacks.
Persons who successfully treated their periodontal disease have also been shown to experience improved cholesterol levels and demonstrated lowered blood pressure. Most readers will recognize these as factors frequently associated with cardiovascular disease.
The bottom line: while we generally don’t hesitate to snap on a seat belt because it may save our lives, not enough of the population understand that oral health basics save more lives than buckling-up! Added benefits? Saving teeth (which leads to better digestion and less need for heartburn medications), fresher breath, and avoiding painful toothaches or complicated dental procedures — which also translates to more dollars in your pocket.
In an ideal world we wouldn’t get cavities, have gum problems, or ever lose a tooth. Perhaps, the world might not be ideal, even then, but at least we wouldn’t have those problems.
Unfortunately, it is a fact of life that many people do lose their teeth – either to tooth decay or periodontal disease – and then require tooth replacements. Despite the growing popularity and acceptance of dental implants as prosthetic tooth substitutes, removable dentures still constitute the most common solution to missing teeth.
If a person still has some natural teeth, they may get what we term a “removable partial denture.” If they have lost all of their teeth, typically they will get a full denture. A commonly observed problem, however, is that once the dentures are made, patients tend to wear them far beyond the point where the denture continues to function well. A little background regarding the problem with dentures may help clarify why this is so:
Some people think that if they get rid of all of their teeth and get dentures they will finally see an end to their dental problems. This is far from reality. Actually, what happens is that patients simply trade one set of dental problems for another. While many patients will tell you that they eat just fine with their dentures, it has probably been so long since they had their real teeth, they have forgotten what it is like to eat normally.
What are some of the disadvantages of wearing dentures?
You lose up to 50% of your biting force.
A full upper denture covers your palate and interferes with your ability to taste your food.
Dentures can move when you eat, speak, cough, or sneeze.
Food accumulates around your dentures after a meal.
Sore spots can develop when the hard denture rubs against your gums.
Patients with an active gag reflex may not be able to even wear a denture without feeling as though they will gag.
Multiple relines of the denture may be required as the shape of your mouth changes. This can happen as a result of gaining or losing weight, or as a result of bone shrinkage and aging.
Atrophy of the upper or lower jaws can make it impossible to develop suction with the denture.
How long do they last?
This is an interesting question, because it is not unusual to encounter patients who tell you their denture was made twenty or even thirty years ago. Believe me, at that point, they are seldom good-looking dentures! But it underscores something about denture wear that is not well understood.
Once a denture is made and, assuming it fits well at the time of delivery, most patients expect – and can experience – good retention and stability.
But the key point is – once made – the dentures don’t change. Yet your mouth can – and often does. New medications can also cause your mouth to become dry, leading to irritation and sore spots. Osteoporosis could lead to shrinkage of the jaw. Despite these changes, many patients attempt to make up for new problems with denture adhesives. Unfortunately, this can open the door to even more irritation, and denture creams containing zinc have even been linked to other health problems such as numbness, tingling and muscle weakness.
While relines can assist with these changes and correct the fit of your denture to improve retention, many patients would do well to consider re-making their dentures after about five years to seven years. In my experience, waiting too long beyond that time period can make the transition to a new denture more difficult.
200 Year-Old Denture
When the change is minimal, such as one might expect after about five years, the transition is generally quite easy. It also helps to have a spare denture for those “oops!” moments. Over the years, I have experienced patients dropping dentures into the sink while cleaning them, accidentally dropping them into garbage disposals, having dogs and cats chew them, and more. Patients will bite into hard objects and break a tooth, they take them out at night and sometimes sit on them, they get stepped on – and one, believe it or not, was even stolen! That was simply too strange a story to recount here.
If your denture is over five years old, talk to your dentist about whether it is time to reline or remake your denture. You will be glad you did.
Dr. Richard Walicki is a dentist practicing general and cosmetic dentistry. While we hope you find the information contained herein interesting and useful, this blog is for informational purposes and is not intended to diagnose any oral disease. Dental conditions should be evaluated by your dental health professional or a qualified specialist.
Search by Topic
Get Access To The AWESOME Health Course
In this 12 week program, you’re going to discover how to achieve AWESOME health and double your energy with natural, tested, and scientific strategies. Just click on the image below: