Remember that gleaming crown, your loyal guard against the gnashing jaws of fate? Well, beneath its gleaming surface, a cunning villain may be plotting your tooth’s downfall: the insidious open margin.
Imagine this: instead of a tight partnership, your crown and tooth have a tiny gap, a secret handshake reserved for troublemakers. Bacteria, those microscopic mischief-makers, throw a perpetual picnic in this hidden nook, nibbling away at your precious tooth like miniature termites. You might not feel their tiny chompers, no immediate twinges, just the illusion of dental safety. But trust me, the party’s on, and the guest list includes cavities, infections, and even bone loss – all whispering sweet nothings of toothlessness in your ear.
So, why does this silent saboteur slip through the cracks? Several sneaky suspects come to mind:
Time’s tiny pickaxes: Years of chomping and grinding can chip away at your tooth, creating tiny crevices where the once-faithful crown no longer fits snugly.
Trauma’s unwelcome nudge: A misplaced bite, a rogue popcorn kernel, even a good-natured tumble can nudge your tooth ever so slightly, turning your crown into a loose-fitting disguise.
The disappearing glue: Sometimes, the cement anchoring your crown can weaken, allowing it to peek-a-boo with your gum line, leaving a doorway for trouble.
The unseen accomplice: And in some cases, the open margin was there from the start, a tiny misstep in the dental dance, undetected and ready to cause mischief.
But here’s the good news: this isn’t a one-way ticket to toothless oblivion. You can shut down the bacteria bash before it turns your pearly whites into a party zone! All you need is a thorough checkup with your dental detective (that’s your dentist!) and a proactive approach.
Remember, ignoring an open margin is like ignoring a leaky roof. You might not see the immediate damage, but the long-term consequences can be a flood of trouble. Replacing the crown, while it might seem like an unnecessary expense, is actually an investment in saving your tooth – and potentially saving yourself thousands down the line.
Think of it this way: a new crown costs a couple of grand. Extraction, bone grafting, and an implant? That’s easily double or triple the price. And let’s not forget the emotional toll of losing a tooth, the impact on your smile, your confidence, your daily life.
So, the next time your dentist mentions an open margin, don’t brush it off as a minor hiccup. Remember, it’s an undercover culprit, a wolf in sheep’s clothing for your dental health. Embrace the proactive approach, get that crown replaced, and send the bacteria packing. Your smile – and your wallet – will sing your praises!
Many people believe that since they aren’t experiencing dental symptoms – like tooth pain or bleeding gums – then all must be well.
Unfortunately, a sizable number of dental problems, including cavities and periodontal disease (bone loss around your teeth), just don’t produce obvious symptoms in their early stages. At least not symptoms that tend to be obvious to patients.
In fact, by the time people the average person experiences pain, his dental issue is typically pretty far along. And all too often, by then, the problem can also be quite expensive to handle.
It might amaze you to discover the types of problems your average dentist encounters every week, many of which you would expect to be painful, but they just aren’t. They can still result in tooth loss though.
Pretty much anyone who has ever worked in a dental office for any length of time will tell you this is so. And they will tell you that you can inform some people that they have a problem, but unless it is “real” to them, they just won’t do anything about it.
They may come back a few years later (or maybe sooner) – usually with an emergency – desperately wanting to save the tooth that you told them about earlier. Of course, by now, it may be too late. And very often they will have forgotten it was ever discussed at all, because it was never a realistic problem for them to begin with.
Human nature can be funny that way.
So, keeping that in mind, it’s generally a good idea to get checked out by a dentist. Regularly.
The best news you can hear is that everything looks great.
But sometimes getting a confirmation that you don’t have cavities or gum disease is not the only reason to get a dental exam. Over the years, I have detected cancer (not just oral cancer) – as well as a host of other non-dental problems – that might have been overlooked had the patient not scheduled an exam. Obviously, we refer patients to an appropriate specialist for treatment when we discover medical problems outside the scope of dental practice.
Other benefits of getting a dental exam: I can recall many patients who told me that what they thought were unrelated health problems simply resolved when their oral problems were gotten under control. These have included digestive problems, low energy problems, elevated blood cell counts, hypertension, and more.
Over the years, some people have told me they don’t want to get a dental exam because they don’t want to discover they have any problems. I guess that works.
Just maybe not too well.
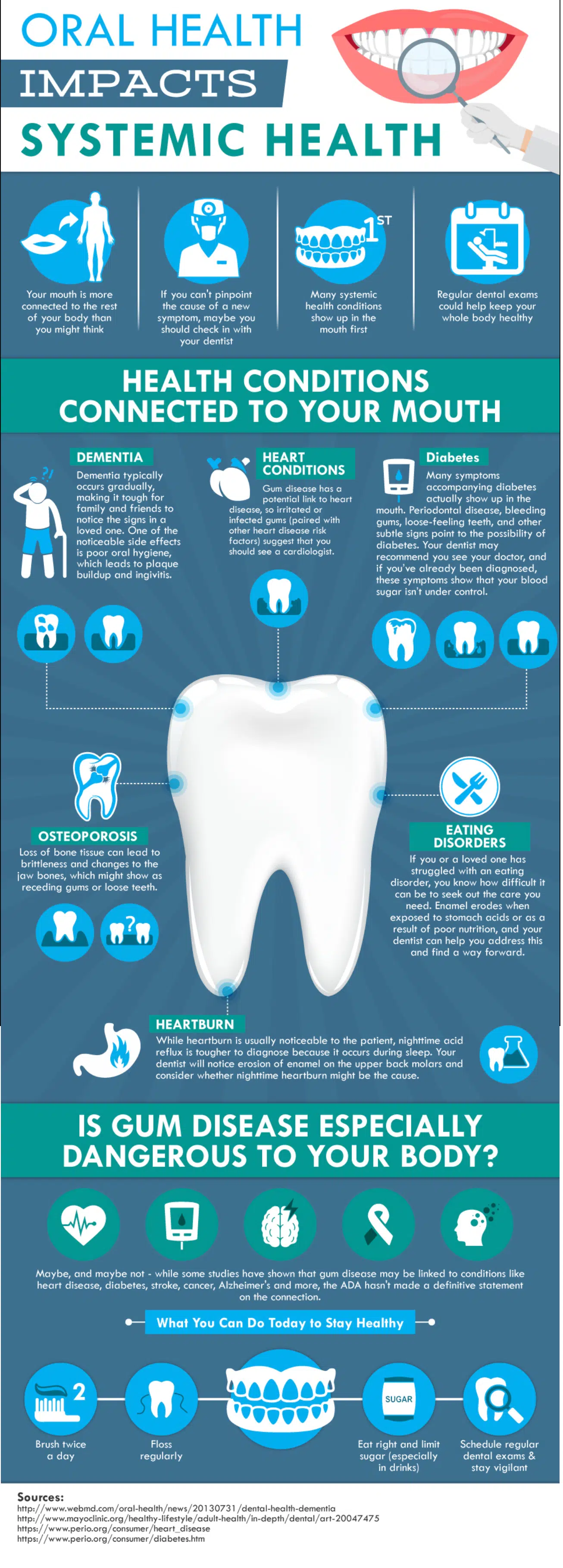
Your overall health is connected to your oral health. Take a look at this infographic. Then think it over. . . .
Because tooth-loss so often creates long-lasting and generally negative effects for personal health and, not infrequently, appearance – the entire array of tooth replacement options has long been an important subject in the dental field. Dentists not infrequently discuss which options are best for their patients, given different circumstances. And if there is any debate in the profession at all, you can be sure the public will also question which options make the most sense for them.
The truth is there is no one right answer. Each person’s circumstances differ – whether the reasons are anatomic, functional, emotional, or financial.
But the question is still an important one to ask, because patients face new realities when they lose even one tooth. These changes include (but are not limited to):
Difficulty chewing
Altered speech
Food impaction
Jaw pain
Drifting teeth
And, then there are the secondary effects:
Poor health resulting from a changing diet
Compromised appearance
Self-consciousness/embarrassment
An inability to wear dentures
Financial challenges created by the need to address these problems
It is this last point that I want to touch upon here, because I have observed a good deal of confusion surrounding dental implants. As a dentist, I am obligated to review all options with an individual when discussing their tooth replacement options – regardless of affordability. I can’t, and don’t, pre-judge anyone financially when discussing their choices.
Commonly, though, when I raise the subject of dental implants, I get an immediate reaction along the lines: “Oh, forget it. I could never afford that. How about a bridge?”
Now, I’m not going to try to convince you that implants are cheap. Restore a full mouth with dental implants and it is likely to be costly. Nevertheless, cheap is relative. For some of my patients, even a small filling can be perceived as expensive. For my wealthy patients, they might be prepared to spend any price for what they perceive will serve them best. Lucky them. Right?
What I hope to do here, however, is to show you when an implant may make the most sense for a person. And — at least, when when it comes to replacing a single tooth — a dental implant may just be the way to go.
But first, permit me to remind you again – there is no one right answer for everybody. Your choices may be very different depending upon whether you are 25 or 85 years old, for example.
I’m sure you can fill-in still other reasons that affect your decision-making process. But for now, let’s consider the following scenario:
A patient loses one tooth.
For the sake of argument, we’ll call it a lower right first molar. Suddenly, the patient realizes this is annoying. Their bite is changing; their gums are sore. They feel the need to do something. Now.
Here are a few options. I’m just going to list the main ones, but there are sub-sets to some of these:
Do nothing anyway.
A removable denture.
A non-removable bridge,
A dental implant.
For the purposes of this discussion, the patient has already decided that doing nothing isn’t working for them.
So, the next option is a removable denture. I usually get “the face” on this one.
And with good reason. Food gets caught around partial dentures every time you eat. You will have to remove the appliance after EVERY meal and clean it separately from your own teeth. Certain foods will also cause it to dislodge as you eat, allowing some of the food to get caught between the denture and your gums. The cost – depending upon what kind of partial you have made – will typically range between $750 and $1,500.† The recommended replacement time: every 5 to 7 years. The reality – people replace them roughly every 15 years. Sometimes more. The longer they put off the replacement though, the more issues they may face with the replacement.
Bottom line: Removable dentures are potentially uncomfortable. Average lifetime replacement cost if you are 25 years old, (based on an average life expectancy of about 79 years, and an average 10-year replacement rate – not adjusting for inflation) is going to be nearly $7,000.
Next, we’ll take up considering a “bridge.” It’s called a bridge because it spans a gap (like a bridge spans a body of water) with a fake tooth, or teeth, in between the ones that are still there. The trouble is that you must shave down the supporting teeth to little stubs so that the result will look natural and be strong enough to take the force of daily chewing. For the most part, bridges look, and can often feel like, your natural teeth; but you do have to floss under the fake tooth after every meal. Food will get caught under there, whether you perceive it or not. If you don’t clean it regularly, the life expectancy of your bridge will be shorter.
Now, the cost on this option can really be widely variable, because some teeth need to have fillings replaced before they can be used as supports for the bridge. In other cases, the teeth may end up with root canals if the process of shaving them down results in lingering sensitivity. This doesn’t always happen, but it is a risk. If the tooth needs that additional treatment it will cost you more.
The average cost to replace a single tooth with a bridge is about $3,500. Again, that can be a little more, or less, depending upon what part of the country – or even what part of a city, you live in.
If, on the other hand, you also need to place or replace fillings on the teeth being used as supports, and you need to do root canals as well, it could be as much as $7,000.
Roughly, double.
The average lifetime replacement cost with the same parameters given above (25 years old with an average life expectancy of 79 years and a 10-year average replacement rate) is going to be: $31,500. And that assumes that the underlying teeth will be strong enough to survive that many replacements.
That brings us to dental implants.
Here is the breakdown: The average implant cost in many metropolitan areas is around $1,800 – $2,200. If you end up needing a bone graft before the implant can be placed, though, add another $550. (Basically, a graft is adding bone to your jaw when you don’t have enough for the implant.) So far, these costs are just for the implant. It doesn’t include the cost of the crown. Add about another $2,100 for the parts needed to make up what supports the crown above the gumline, and the crown itself. If your tooth is short, and there isn’t enough tooth height to which your crown can be easily cemented, you might need something called a UCLA abutment — it lets your dentist screw down the crown instead of cementing it. That could cost you more. How much depends upon the lab your dentist uses, but $500 more wouldn’t be unusual.
On the low end, one implant may cost $3,900. On the high end, let’s round up to $4,900.
So, what about the average lifetime cost?
$4,400.
That’s less than either partial dentures or bridges!
Why?
Because, unless you bite into a rock, grind your teeth uncontrollably, or have some serious illness that causes you to lose bone around the implant – any of which can happen to you with the other options as well – you will probably have your implant for life. Still, no one can guarantee this because, sometimes, plain ol’ dumb luck will factor into any equation.
But, you can’t get a cavity on an implant. On the other hand, you still can get a cavity on the teeth that support your partial denture, or bridge (and crowns, for that matter).
So, do the math. Look at your circumstances, and decide what is right for you. But when your dentist starts talking to you about dental implants, hear them out. It just might be more cost effective than you realize.
† [Note: The prices mentioned here are just averages in US Dollars at the time of this writing. Actual costs could be more, or less, depending upon where you live.]
Common sense. Does it seem to you that this has become a rare commodity nowadays? Possibly, then, it is really uncommon sense that we should be talking about.
The latest example of an affront to logic – at least for me – lies in the latest media challenge to oral health. This morning various news agencies including The New York Times, suggested that maybe flossing is really overrated. Apparently, “officials” have never researched the effectiveness of regular flossing.
Now, millions of people are likely to jump on this as a justification for not flossing. But, in reality, the new media sensation is probably not going to change very much at the end of the day. Why? Because I can confidently tell you – based on more than 25-years of personal experience – most people don’t floss anyway. About all this latest “research” will promote is the possibility that some people will feel just a little less guilty about what others with any sense (common or uncommon) already understand is a pretty good idea.
But, it makes for good press. Doesn’t it?
Just for the sake of argument, let’s assume that flossing doesn’t remove plaque. Heck. Some people fail to remove plaque with a toothbrush. That doesn’t mean either fails to benefit the patient, if done properly. I can think of several reasons why flossing helps, though:
Passing floss between the teeth sweeps out the contact point between them – meaning the points where they touch. That’s a source of about 30% of all tooth decay. Your toothbrush typically doesn’t reach those areas, unless you have gaps between your teeth. Floss does reach those areas.
Flossing stimulates blood flow in the gums. One of the body’s first-line mechanisms of defense is to increase blood flow to an affected area. You are effectively helping your body do this in a controlled manner by flossing.
A number of the bacteria under your gums are anaerobic bacteria. That means they don’t grow in room air. So what is a person introducing into the gum pocket when they pull back their gums by flossing? Could it be . . . air? Is it possible that the oxygen in the air could kill some of those bacteria as well?
Think about it.
If we can set aside this newly created question of doubt for just a moment, I would propose that you ask yourself the following question:
“Have I ever flossed consistently?”
By this, I mean every day, and it would have to have included doing so for at least two weeks.
This question is particularly directed to someone if they ever had a gum problem like gingivitis or periodontal disease. Sure, one needs to get rid of tartar and control bacteria as well, but for patients that make the effort to floss (and with only a few qualifications that I can think of), it is almost a sure bet that their gums got better as a result of the daily exercise. First of all, the gums probably bled less afterward. Not in the beginning – to be sure – but after about two weeks of flossing every day, we typically see positive change. Breath improves too. An overall sense of well-being is not out of the question either.
When it comes to flossing sporadically, I agree. It doesn’t help much. It’s kind of like exercising once or twice a month. And let’s face it, that’s where most of the population lives when it comes to flossing — once in a blue moon. Is regular exercise effective, though? What does your common sense tell you?
Why would I hold on to this idea in the face of “new evidence”? Well, I have seen flossing help too many times to just call it a coincidence. Hard core scientists might say “Oh, well, that’s just anecdotal evidence. It doesn’t stand up to real scientific scrutiny.” OK. Then survey practicing dentists. Let’s see if I’m the only one with that observation and experience. I doubt it.
I’m not saying flossing is the only thing you need to do to have healthy gums. It isn’t. Diet and good nutrition are paramount. A healthy immune system doesn’t hurt either. But for Pete’s sake, flossing is cheap, really not all that hard to do once you have practiced it for a while, and it can end up saving you a lot of money in the long run. With health care costs being what they are, I can’t think of too many actions a person can take that bear as much fruit and keep money in their pockets.
But, if the media has just succeeded in making you feel better about not flossing, then OK. Bully for them. (Heaven knows, they do a top notch job spending most of their time getting people to feel less than great.)
And, I suppose there are other ways to handle tooth loss – which, by the way, happens a lot more from gum disease than tooth decay.
I have little doubt that some patients who visit a dentist and are told they have decay, but don’t experience any symptoms, are convinced that someone is trying to pull the wool over their eyes. There are probably several reasons for this. Possibly, they had been to some unscrupulous person in the past who suggested they had a problem, when they really didn’t.
I can see how that might create skepticism. I mean, it’s conceivable that sort of thing could happen.
But even if that were the case, I sincerely don’t believe it represents the behavior of a majority of dentists. Most of the dentists I know genuinely care about what they do and the people they treat. So maybe these skeptics are just people who don’t trust anyone. I don’t know.
The reality, though, is that these patients will eventually be in for a big surprise when the you-know-what hits the fan. Or – and let’s keep this a family column — when the decay hits the nerve.
But that could take a while.
And I believe that could be where some of the problem lies. A patient tries to use this to their advantage — they want to buy some time. After all, it’s not really being a “problem” for them in that they don’t perceive anything as being different. When the problem eventually does occur, I usually hear: “I never thought it would happen to me.”
A doctor detecting treatable decay usually recommends that the patient handle it at their earliest opportunity.
Why? Well, the patient can catch the problem when it is small, when it is less likely to cause post-operative discomfort, and when it will generally cost them a lot less.
But, first, let’s back up a little and explain why it’s possible to have a cavity – several in fact – and have absolutely no symptoms.
Most decay starts on the outer surface of the tooth called the enamel. It’s roughly 97% mineral in consistency and does not contain nerves. That means it has no feeling. Practically zero. Your dentist could DRILL on that part of the tooth and most of the time you won’t feel it.
Notice that in the earlier paragraph I mentioned “treatable” decay. Well, when would decay not be treatable right away? I can’t speak for other dentists, but I typically won’t treat decay when it is confined to the enamel. Why? It has the potential to re-mineralize. In other words, it has the capacity to fix itself – that is, if you don’t continue to do the things that led to the cavity in the first place. Usually, this is related to your diet, but it can be affected by hormones, or even medications.
Why not mention home care first? Isn’t that important too? Of course it is. It just may not be the most important factor.
Another time a dentist might not treat a cavity could relate to the age of the patient. For a much older patient, there are times when the pain or infection are not likely to come up before the patient passes. Of course, your dentist doesn’t have a crystal ball on that point. (Well, probably not.) But, it wouldn’t make sense to recommend treatment in the majority of those cases.
And this takes us back to the nature of a cavity. They often take a long time to get bigger. (But not always…. Again, no crystal ball here.) The reason has to do with the hardness of the enamel itself. Enamel, for you trivia lovers, is the hardest substance in your body. It’s harder than bone, and that property, along with the lack of sensation, can be problematic.
Here’s why: a cavity is often quite small on the outside of the tooth. It’s actually difficult for decay to work its way through that hard enamel. Most of the time it burrows a narrow channel down to the dentin (only a couple of millimeters away) and then it really starts to spread. Because dentin is softer than enamel, it’s just easier for it to spread more quickly there. By the way, this additional, and deeper, decay – very often still doesn’t hurt – as long as it is far enough away from the nerve.
Meanwhile, your enamel is, for the most part, continuing to hold its form. That stuff is hard. But things are generally hollowing out on the inside of the tooth now — out of sight and out of mind — as the decay continues to spread. Painlessly.
Eventually, your tooth can become very much like an eggshell.
Then one fine day you bite on something, and the hard enamel that was still doing its job holding the form of the tooth caves into the hole below. It just got too thin.
Now, at this point, does the skeptic understand that he got a cavity? Sure. Some of them finally get it. But for others –no! It’s more like: “Hey that blowhard dentist was obviously wrong because he talked about me having cavities years ago, and look – I did fine until now. In fact, I probably just lost a filling! Jeez, this hole just came out of nowhere. It’s probably the fault of some earlier dentist.” (Um, Mr. Skeptic never got the filling though. Remember?)
“Hey doc, how much is this going to cost me? $2,400?!!! (For a root canal, buildup and crown.) Are you insane? Just pull it.”
Now you are going to be missing a tooth, and may lose even more teeth as a result. Yet, when the doc first mentioned it, that cavity was only going to cost $150. How can it suddenly become sixteen times more expensive?!
“Rip-off artist. Seems you can’t trust anyone. . . .”
Dr. Richard Walicki is a dentist practicing general and cosmetic dentistry. While we hope you find the information contained herein interesting and useful, this blog is for informational purposes and is not intended to diagnose any oral disease. Dental conditions should be evaluated by your dental health professional or a qualified specialist.
Search by Topic
Get Access To The AWESOME Health Course
In this 12 week program, you’re going to discover how to achieve AWESOME health and double your energy with natural, tested, and scientific strategies. Just click on the image below: