I have little doubt that some patients who visit a dentist and are told they have decay, but don’t experience any symptoms, are convinced that someone is trying to pull the wool over their eyes. There are probably several reasons for this. Possibly, they had been to some unscrupulous person in the past who suggested they had a problem, when they really didn’t.
I can see how that might create skepticism. I mean, it’s conceivable that sort of thing could happen.
But even if that were the case, I sincerely don’t believe it represents the behavior of a majority of dentists. Most of the dentists I know genuinely care about what they do and the people they treat. So maybe these skeptics are just people who don’t trust anyone. I don’t know.
The reality, though, is that these patients will eventually be in for a big surprise when the you-know-what hits the fan. Or – and let’s keep this a family column — when the decay hits the nerve.
But that could take a while.
And I believe that could be where some of the problem lies. A patient tries to use this to their advantage — they want to buy some time. After all, it’s not really being a “problem” for them in that they don’t perceive anything as being different. When the problem eventually does occur, I usually hear: “I never thought it would happen to me.”
A doctor detecting treatable decay usually recommends that the patient handle it at their earliest opportunity.
Why? Well, the patient can catch the problem when it is small, when it is less likely to cause post-operative discomfort, and when it will generally cost them a lot less.
But, first, let’s back up a little and explain why it’s possible to have a cavity – several in fact – and have absolutely no symptoms.
Most decay starts on the outer surface of the tooth called the enamel. It’s roughly 97% mineral in consistency and does not contain nerves. That means it has no feeling. Practically zero. Your dentist could DRILL on that part of the tooth and most of the time you won’t feel it.
Notice that in the earlier paragraph I mentioned “treatable” decay. Well, when would decay not be treatable right away? I can’t speak for other dentists, but I typically won’t treat decay when it is confined to the enamel. Why? It has the potential to re-mineralize. In other words, it has the capacity to fix itself – that is, if you don’t continue to do the things that led to the cavity in the first place. Usually, this is related to your diet, but it can be affected by hormones, or even medications.
Why not mention home care first? Isn’t that important too? Of course it is. It just may not be the most important factor.
Another time a dentist might not treat a cavity could relate to the age of the patient. For a much older patient, there are times when the pain or infection are not likely to come up before the patient passes. Of course, your dentist doesn’t have a crystal ball on that point. (Well, probably not.) But, it wouldn’t make sense to recommend treatment in the majority of those cases.
And this takes us back to the nature of a cavity. They often take a long time to get bigger. (But not always…. Again, no crystal ball here.) The reason has to do with the hardness of the enamel itself. Enamel, for you trivia lovers, is the hardest substance in your body. It’s harder than bone, and that property, along with the lack of sensation, can be problematic.
Here’s why: a cavity is often quite small on the outside of the tooth. It’s actually difficult for decay to work its way through that hard enamel. Most of the time it burrows a narrow channel down to the dentin (only a couple of millimeters away) and then it really starts to spread. Because dentin is softer than enamel, it’s just easier for it to spread more quickly there. By the way, this additional, and deeper, decay – very often still doesn’t hurt – as long as it is far enough away from the nerve.
Meanwhile, your enamel is, for the most part, continuing to hold its form. That stuff is hard. But things are generally hollowing out on the inside of the tooth now — out of sight and out of mind — as the decay continues to spread. Painlessly.
Eventually, your tooth can become very much like an eggshell.
Then one fine day you bite on something, and the hard enamel that was still doing its job holding the form of the tooth caves into the hole below. It just got too thin.
Now, at this point, does the skeptic understand that he got a cavity? Sure. Some of them finally get it. But for others –no! It’s more like: “Hey that blowhard dentist was obviously wrong because he talked about me having cavities years ago, and look – I did fine until now. In fact, I probably just lost a filling! Jeez, this hole just came out of nowhere. It’s probably the fault of some earlier dentist.” (Um, Mr. Skeptic never got the filling though. Remember?)
“Hey doc, how much is this going to cost me? $2,400?!!! (For a root canal, buildup and crown.) Are you insane? Just pull it.”
Now you are going to be missing a tooth, and may lose even more teeth as a result. Yet, when the doc first mentioned it, that cavity was only going to cost $150. How can it suddenly become sixteen times more expensive?!
“Rip-off artist. Seems you can’t trust anyone. . . .”
OK. So let’s say it has been decided: you are a candidate for an implant.
Now what?
You may have heard that getting an implant can take a long time. By contrast, you can have a bridge to replace your missing tooth in about two weeks or less. Isn’t that better?
Not so fast. It all depends.
Let’s look at a couple of scenario
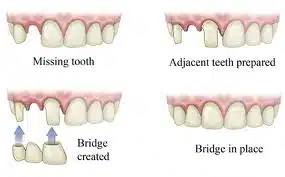
s. If you are replacing only one tooth and have two adjacent teeth here is what you should consider:
In order to place a bridge, you have to shave down those teeth so that they will support the bridge. This limits their longevity and may open the door to the need for additional work, such as root canal therapy in the future.
You should also understand that bridges don’t last forever. The national average, according to university studies and insurance company estimates, is only five to fifteen years. If, you are in your twenties, a bridge can turn out to be much more costly over your lifetime.
Let’s see how this plays out:
For the sake of argument, consider that a person has lost their first molar. The 2013 national average price for crowns (the individual units that make up a bridge) was about $1160. Since our hypothetical bridge has three units, that adds up to $3,480. If existing fillings need to be replaced due to decay, it could cost another $500. And if a root canal is needed because the filling is now closer to the nerve, this can cost as much as another $1,100 for a molar. Suddenly, the total bill can exceed $5,000 using our example.
In five to fifteen years the bridge may need replacement. Let’s be generous and say it lasts fifteen. Between the ages of 25 and 85, that’s four replacements – nearly an additional $14,000 – if nothing else is needed.
In the long run, replacing one tooth using a bridge can cost nearly $20,000 over your lifetime. And that’s assuming it is still in a condition that permits a new bridge.
What if instead we replace the tooth with an implant? At today’s rates, a traditional root form implant runs between $1,800 and $2,000 in my area. An abutment (that’s the part which ties the implant and the implant crown together) will range in price from an average of $850 to $1,200. Prices for implant crowns vary widely – though many dentists charge the same fee as they do for regular crowns. In this example, we’ll use the fee given above, so $1,160.
If we take the higher estimates here, we’re up to $4,360. That’s only $880 more than our bridge in the earlier example’s “best case” scenario.
The difference? That implant (barring situations like an accident causing physical injury to the implant) has a good chance of lasting a lifetime. That’s a lot less than $20,000 over time if you go the bridge route.
I have had patients react in various ways to this analysis. Some tell me “I really don’t want to wait three to nine months, while wearing a temporary partial, for the implants to be ready.” Others have said, “Well, if I’m going to have to replace a bridge down the road, or even end up with an implant later anyway – I might as well just do it now.”
Both arguments have their merits. But at least now you have some information that can help you make an informed choice.
No matter how you slice it, tooth problems can be a pain. Among these, cracked teeth stand out for their confusing and erratic nature. A cracked tooth can be painful, annoying, and an exercise in frustration for patients and dentists alike. While there can be many factors that contribute to cracked teeth, the bottom line is that if your tooth is cracked the solution is often involved, potentially expensive — and, despite best efforts, tooth loss is still a very real possibility. Clicking on the picture below will take you to a compilation of questions and answers about cracked teeth. It covers a lot of ground, but if you think you may have a cracked tooth, it is worth reading so that you can know what to expect.
Let’s face it: seeing a doctor – any sort of doctor – can be expensive. And dentists are no exception. But if a person’s diet and home care have been lacking, the cost of dental treatment can quickly sky-rocket. One of the problems with dental care has to do with the fact that many patients still suffer from the idea that if they don’t feel anything wrong with their teeth, then all is well.
Unfortunately, when it comes to teeth, most people miss the boat entirely with this concept. The reason is simple: the outer part of the tooth – the enamel – is mostly mineral and has no nerves. That means you can have a cavity and not know it. Several, actually. Most dentists will attest to the fact that many patients are shocked to learn they have any cavities at all.
The trouble is that by the time a cavity actually gets big enough to pose a problem, it’s a PROBLEM. For most people that trouble is spelled P-A-I-N.
It’s really no small wonder that so many individuals associate going to the dentist with toothaches. For those patients, it is the only time they will actually make an appointment. They go because they now know they have a cavity. Pain is a huge motivator. . . .
By the time a tooth hurts, though, the cavity is usually pretty close to the nerve. This means that if there is still enough tooth structure left to work with, the dentist may consider a root canal to remove the source of the pain – in other words – the nerve. Usually, this is not cheap. A root canal on a molar can cost over a thousand dollars when performed by a specialist. Then the patient has to go back to the dentist to have the tooth built up again (because so much tooth structure was lost to decay) and finally, the tooth may even need a crown. Lacking a blood supply and nerve thanks to the root canal, the tooth is now brittle and can break. Since your back teeth get a lot of pressure when you chew, failing to crown it may result in the tooth cracking and all that money you spent on the root canal goes out the window.
In a number of cases, because many people simply fear getting a root canal (not because they actually had one, but because they heard that a friend of a friend had a bad experience, and they never want to go through THAT), they opt to remove the tooth instead.
But now they have to replace the missing tooth or else their teeth will shift around and their bite goes awry. And fixing that new problem typically costs even more!
It can be frustrating.
Many people figure no one will see a missing back tooth, so why not pull it, since that is cheaper? At least they think so – until they notice their front teeth starting to form gaps, and find that food gets stuck all over the place whenever they eat. But then again, what if it’s a front tooth that needs to go?
You possibly think: “Wow, this is a problem, but I still really need to find something cheap.” OK, then. If you live in Philadelphia, you may Google “affordable Philadelphia dentist” or “cheap dentist.” A number of listings for dental implants appear, maybe some for “affordable cosmetic dentistry.” Wow, this isn’t sounding at all affordable!!! Wait! A couple of dental schools come up too. “Hmmm. Do I really want someone in their first year of dental clinic restoring my front tooth? It will be less expensive. But, then again . . . .”
The affordable dentist is someone who will understand your situation and can help you to find a workable solution for your circumstances. Many offices offer low-cost or interest-free programs that help you get the work you need today and then spread payments out over time. In some cases, it may be helpful to set up a lay-away program, especially if you have specific needs for which you have been given an estimate of treatment costs. In this manner you won’t end up spending your money on other less-essential items. Many offices will assess a minor fee to manage this plan, but it is usually quite small.
In the meantime, it is essential to keep yourself out of trouble with good preventive dental practices. Learn what diet has to do with your teeth and which home care habits are best. Remember, when it comes to teeth and gums, “no pain” most definitely does not always mean “no problems”.
Recently, I saw four new patients in my dental office during a given week. All four of those patients scheduled their visits because they perceived pieces of their tooth chipping away. In three out of four of those cases, the offending tooth was so badly decayed that the tooth couldn’t be saved. Yet only one of those patients came in with any discomfort.
The common thread in each of these cases is that the patient waited until the tooth was actually breaking apart to seek dental care. All too often, the trigger that brings people to the dentist is pain. Yet here, we had at least three cases where pain was not a factor and yet the tooth was decaying.
How is this possible?
A little understanding of dental anatomy helps here. The outer layer of teeth, the enamel, is the hardest substance in your body. Because its composition is predominantly mineral, it is possible to have decay throughout that layer without experiencing any sensation. In fact, it is even possible for your dentist to drill that part of the tooth (in most cases) without pain. The next layer under your enamel is called dentin. Decay can travel into the dentin – where it usually spreads more quickly, because it is not as hard – and a person still may not experience pain.
By the time a tooth that is decayed hurts, the decay has generally travelled so far that it nears the innermost layer – the pulp. The pulp contains nerves and blood vessels – so, naturally, pain becomes a factor. If a patient is lucky enough to have enough tooth structure remaining, chances are that the tooth will need a root canal if it is to be saved. Otherwise, extraction is the usual alternative.
One lost tooth can lead, in turn, to still other dental problems. Most notably these include shifting teeth, TMJ problems, periodontal problems, cosmetic difficulties or simply difficulty chewing. It may even lead to the loss of more teeth – not to mention the fact that tooth replacement options can become rather expensive.
Hopefully, just understanding that a lack of pain does not equate to a lack of problems will prompt some readers that haven’t seen a dentist in a long time to do so. Sometimes people fear learning that they have cavities that need to be treated, and so they put off the examination. Consider, however, that it is better to learn you have five teeth that need fillings, than to learn you have several that have to be extracted.
Dr. Richard Walicki is a dentist practicing general and cosmetic dentistry. While we hope you find the information contained herein interesting and useful, this blog is for informational purposes and is not intended to diagnose any oral disease. Dental conditions should be evaluated by your dental health professional or a qualified specialist.
Search by Topic
Get Access To The AWESOME Health Course
In this 12 week program, you’re going to discover how to achieve AWESOME health and double your energy with natural, tested, and scientific strategies. Just click on the image below:

 Now, at this point, does the skeptic understand that he got a cavity? Sure. Some of them finally get it. But for others –no! It’s more like: “Hey that blowhard dentist was obviously wrong because he talked about me having cavities years ago, and look – I did fine until now. In fact, I probably just lost a filling! Jeez, this hole just came out of nowhere. It’s probably the fault of some earlier dentist.” (Um, Mr. Skeptic never got the filling though. Remember?)
Now, at this point, does the skeptic understand that he got a cavity? Sure. Some of them finally get it. But for others –no! It’s more like: “Hey that blowhard dentist was obviously wrong because he talked about me having cavities years ago, and look – I did fine until now. In fact, I probably just lost a filling! Jeez, this hole just came out of nowhere. It’s probably the fault of some earlier dentist.” (Um, Mr. Skeptic never got the filling though. Remember?)