Can a Tooth Infection Kill You? The Scary Truth About Dental Abscesses
People often ask, “Can a tooth infection kill you?” The answer, while alarming, is yes—if left untreated. What starts as a simple toothache can escalate into a dangerous dental abscess that spreads beyond the mouth, potentially becoming life-threatening.
In this post from our Weird Dental Facts series, we’ll explain how dental infections can turn deadly, the warning signs to look for, and what you can do to protect your health.
We’d also love for you to subscribe to our YouTube Channel and share your thoughts. Your feedback helps us create more helpful and entertaining content!
How Can a Tooth Infection Become Life-Threatening?
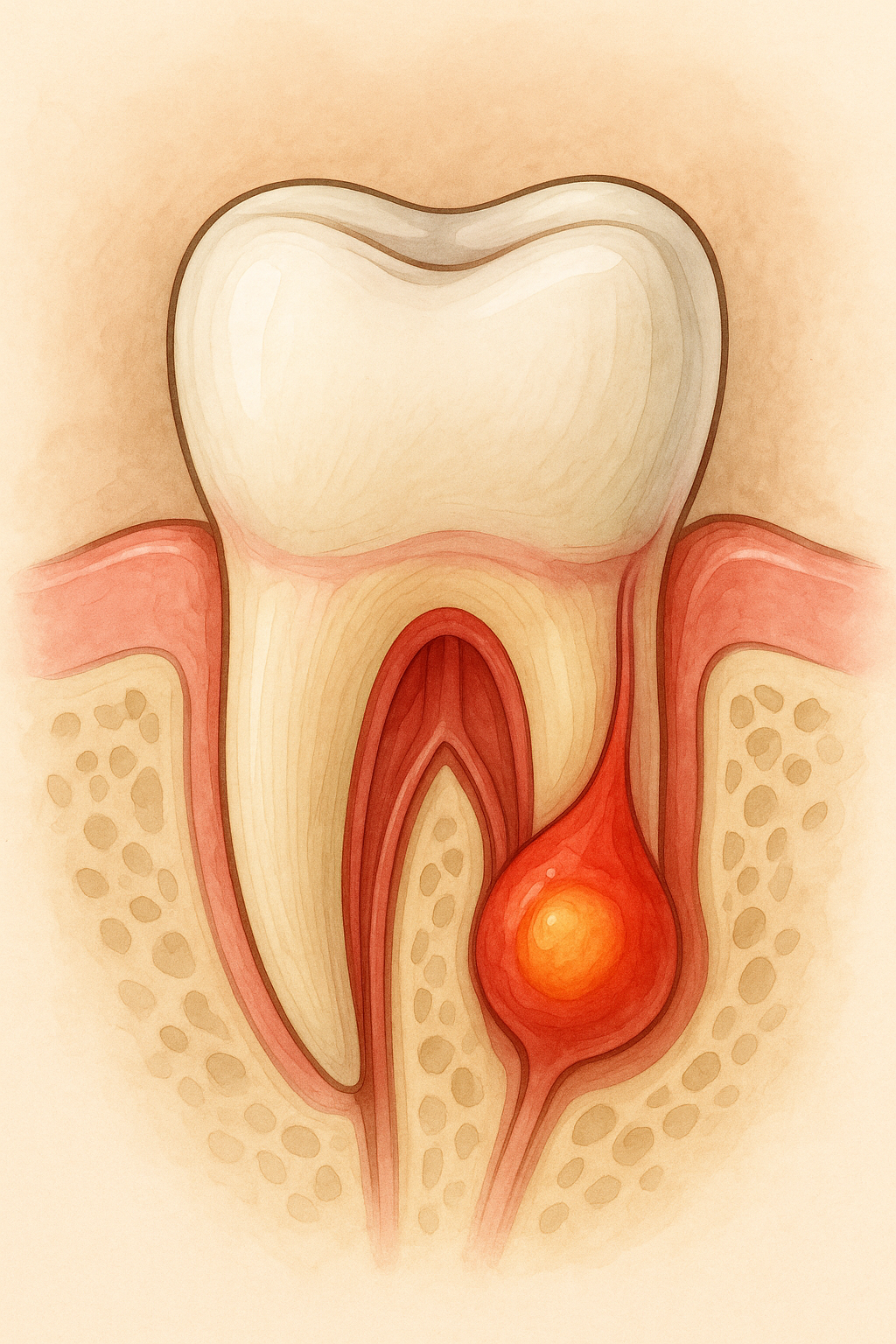
A toothache might feel like a small problem, but if the underlying infection isn’t treated, it can spread. When bacteria enter the inner pulp of the tooth, they can create an abscess—a pocket of pus that may expand into the jaw, face, or even the bloodstream, leading to a condition called sepsis.
Untreated periodontal disease(gum disease) can also lead to abscess formation. The danger is that dental infections are not always painful in their early stages, causing many people to delay treatment until it’s too late.
What Is Ludwig’s Angina?
One of the most serious complications of an untreated dental infection is Ludwig’s Angina. This fast-spreading infection can travel from the roots of the teeth to the floor of the mouth and under the tongue, causing severe swelling. If the swelling blocks the airway or makes swallowing difficult, it becomes a medical emergency.
Immediate medical treatment—such as opening the airway, administering antibiotics, or even surgery—is often required to save a patient’s life. Delaying treatment can be fatal.
How Dental Infections Spread Beyond the Mouth
When bacteria from a tooth infection enter the bloodstream, they can travel to other parts of the body. In rare but severe cases, this can lead to heart infections (endocarditis), brain abscesses, or even sepsis. These complications highlight why early dental care is crucial—what starts as mild pain or swelling can spiral into a medical crisis if ignored.
Signs of a Serious Dental Infection
See a dentist right away if you notice any of the following warning signs:
Persistent or throbbing toothache
Swelling in the face, jaw, or under the tongue
Fever or general malaise
Difficulty swallowing or breathing
A foul taste or pus drainage in the mouth
How to Prevent Dangerous Dental Infections
The best way to avoid asking, “Can a tooth infection kill you?” is to take preventive steps:
Brush and floss daily to remove harmful bacteria.
See your dentist twice a year for check-ups and cleanings.
Limit sugary foods and drinks that feed harmful bacteria.
Boost your immune system with a balanced diet rich in vitamins C and D.
Never ignore a toothache, swelling, or signs of infection—early treatment is much safer and less costly.
FAQ: Can a Toothache Really Be Fatal?
Can a toothache kill you? A toothache itself won’t, but if the infection behind it spreads untreated, it can become deadly.
How fast can a dental infection spread? Some infections can progress in just a few days, especially if they move into the soft tissues of the neck or bloodstream.
What should I do if I suspect an abscess? See a dentist or doctor immediately. Do not attempt to drain it yourself—this can worsen the infection.
Key Takeaway
A tooth infection can, in rare cases, be fatal if left untreated. Don’t take chances with your health—seek professional dental care at the first sign of pain or swelling.
For more surprising dental trivia and health tips, visit our Weird Dental Factsarchive.
How Do I Know If My Tooth Infection Is Spreading?
Wondering if your dental issue is becoming serious? A key sign of a spreading infection is pain that worsens or radiates to the jaw, ear, or neck. Swelling in the face or under the tongue, difficulty breathing, fever, or a foul taste in your mouth are all red flags. If you’re asking, “can a tooth infection kill you?” the answer is that severe infections can become life-threatening if they block your airway or enter the bloodstream. Don’t wait—seek professional help immediately.
Did you know that there are way more bacteria in your mouth than there are people on the planet? By some estimates: 120 BILLION bacteria can grow in 24 hours!
That’s really a lot of bugs!
Germophobes might get a little skittish reading this, so it may make you feel better to know that most of them are harmless.
Typically, the body’s natural defenses and good oral health care — such as daily brushing and flossing — can keep these bacteria in check. However, without proper oral hygiene, bacteria can reach levels that might lead to oral infections, such as tooth decay and gum disease. After more than twenty years of practice I have also observed that oral health can act as a window to your overall health.
For example, your oral health might be affected by, may itself affect, or may contribute to, various diseases and conditions — including:
Cardiovascular disease. Some research suggests that heart disease, clogged arteries and stroke might be linked to the inflammation and infections that oral bacteria can cause.
Endocarditis. Endocarditis is an infection of the inner lining of your heart (endocardium). Endocarditis typically occurs when bacteria or other germs from another part of your body, such as your mouth, spread through your bloodstream and attach to damaged areas in your heart.
Pregnancy and birth. Periodontitis has been linked to premature birth and low birth weight.
Diabetes. Diabetes reduces the body’s resistance to infection — putting the gums at risk. Gum disease appears to be more frequent and severe among people who have diabetes. Research shows that people who have gum disease have a harder time controlling their blood sugar levels.
Osteoporosis. Osteoporosis — which causes bones to become weak and brittle — might be linked with periodontal bone loss and tooth loss.
HIV/AIDS. Oral problems, such as painful mucosal lesions, are common in people who have HIV/AIDS.
Alzheimer’s disease. Tooth loss before age 35 might be a risk factor for Alzheimer’s disease.
Other conditions. Other conditions that might be linked to oral health include Sjogren’s syndrome — an immune system disorder that causes dry mouth — and eating disorders.
Because bacteria can proliferate as quickly as they do, we now provide our patients with a way to minimize bacterial risks during their cleaning appointments. We have the ability to use a laser decontamination process that dramatically reduces bacterial levels in your gum pockets painlessly, without the need for anesthesia, and in as little time as 5 to 10 minutes. Better still, the lowered bacterial levels are expected to continue for six to eight weeks.
Unfortunately, dental insurance still tends to be a little behind the times in terms of their coverage for the procedure. We have kept the cost low, however, in order that most patients can benefit from this exciting new technology. You can read more about it by clicking HERE.
There are a number of factors that can contribute to the formation of dental cavities. One fundamental that will apply to most everyone concerns the reduction of dental plaque. If you want fewer cavities, reduce your plaque levels.
Dental plaque can be defined as a complex microbial community, with greater than 10 to the 10th power bacteria per milligram. (That’s really a lot of bacteria.) Just to keep things simple, though, the problem is that these bacteria produce acids on your teeth – and the acids dissolve the enamel, leading to tooth decay.
After only a few years of practice, it became obvious to me that most people have difficulty identifying plaque. Even now, I’ll begin a dental exam or cleaning on a person and start removing large areas of plaque. If I casually ask the patient about their cleaning regimen, often I’m told “I brushed just before I came in here!”
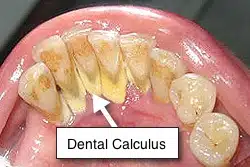
Since that much plaque can’t form in an hour, the obvious conclusion is that the patient missed it or simply doesn’t see it. Just to be clear, plaque is the soft, sticky film that occurs on the surface of teeth – not the hard substance your dentist or hygienist has to pick away, which is tartar. Though it is basically mineralized plaque, virtually no amount of tooth brushing and flossing will remove tartar after the fact (dentists call it ‘calculus’). Once formed, calculus needs to be removed at your office visit.
It is useful to know that if you control your plaque well, calculus won’t be much of a problem. So let’s focus on that for a moment. What do you do if you feel you are brushing, but the dentist tells you he still sees plaque? Stain it!
Lately, I have been seeing more commercials advertising products for children that stain their teeth blue after they have rinsed with it. The child then brushes until all of the blue stain has been removed. What the liquid is staining is plaque. I think this is a great way to simplify the process of identifying the problem. Whether you are six or sixty, the principle is the same.
If you want to be certain you have gotten the plaque off, rinse with the stain after each meal and then brush (and floss) until you have removed the discolored areas. Barring other systemic or external contributory factors (such as medications leading to a dry mouth), you and your dentist should see a big improvement in the cleanliness of your mouth, and fewer cavities over time!
In an ideal world we wouldn’t get cavities, have gum problems, or ever lose a tooth. Perhaps, the world might not be ideal, even then, but at least we wouldn’t have those problems.
Unfortunately, it is a fact of life that many people do lose their teeth – either to tooth decay or periodontal disease – and then require tooth replacements. Despite the growing popularity and acceptance of dental implants as prosthetic tooth substitutes, removable dentures still constitute the most common solution to missing teeth.
If a person still has some natural teeth, they may get what we term a “removable partial denture.” If they have lost all of their teeth, typically they will get a full denture. A commonly observed problem, however, is that once the dentures are made, patients tend to wear them far beyond the point where the denture continues to function well. A little background regarding the problem with dentures may help clarify why this is so:
Some people think that if they get rid of all of their teeth and get dentures they will finally see an end to their dental problems. This is far from reality. Actually, what happens is that patients simply trade one set of dental problems for another. While many patients will tell you that they eat just fine with their dentures, it has probably been so long since they had their real teeth, they have forgotten what it is like to eat normally.
What are some of the disadvantages of wearing dentures?
You lose up to 50% of your biting force.
A full upper denture covers your palate and interferes with your ability to taste your food.
Dentures can move when you eat, speak, cough, or sneeze.
Food accumulates around your dentures after a meal.
Sore spots can develop when the hard denture rubs against your gums.
Patients with an active gag reflex may not be able to even wear a denture without feeling as though they will gag.
Multiple relines of the denture may be required as the shape of your mouth changes. This can happen as a result of gaining or losing weight, or as a result of bone shrinkage and aging.
Atrophy of the upper or lower jaws can make it impossible to develop suction with the denture.
How long do they last?
This is an interesting question, because it is not unusual to encounter patients who tell you their denture was made twenty or even thirty years ago. Believe me, at that point, they are seldom good-looking dentures! But it underscores something about denture wear that is not well understood.
Once a denture is made and, assuming it fits well at the time of delivery, most patients expect – and can experience – good retention and stability.
But the key point is – once made – the dentures don’t change. Yet your mouth can – and often does. New medications can also cause your mouth to become dry, leading to irritation and sore spots. Osteoporosis could lead to shrinkage of the jaw. Despite these changes, many patients attempt to make up for new problems with denture adhesives. Unfortunately, this can open the door to even more irritation, and denture creams containing zinc have even been linked to other health problems such as numbness, tingling and muscle weakness.
While relines can assist with these changes and correct the fit of your denture to improve retention, many patients would do well to consider re-making their dentures after about five years to seven years. In my experience, waiting too long beyond that time period can make the transition to a new denture more difficult.
200 Year-Old Denture
When the change is minimal, such as one might expect after about five years, the transition is generally quite easy. It also helps to have a spare denture for those “oops!” moments. Over the years, I have experienced patients dropping dentures into the sink while cleaning them, accidentally dropping them into garbage disposals, having dogs and cats chew them, and more. Patients will bite into hard objects and break a tooth, they take them out at night and sometimes sit on them, they get stepped on – and one, believe it or not, was even stolen! That was simply too strange a story to recount here.
If your denture is over five years old, talk to your dentist about whether it is time to reline or remake your denture. You will be glad you did.
In today’s challenging economic climate, people find themselves having to make every dollar they spend count. As a result, individuals considering cosmetic dental work face the additional problem of not having such procedures be covered by dental insurance. For some, that puts treatment a little farther out of reach.
While it may be a common perception that cosmetic dental procedures are completely elective, many prospective job seekers have come to realize that having an unattractive smile could make the difference between being hired and being passed over for employment.
One of the most common methods used to improve flaws in a person’s smile has been the use of dental veneers. These are typically thin shells of porcelain that are bonded to the surfaces of a patient’s teeth and can be used to correct a variety of problems: from unsightly old fillings to crooked teeth or chips in the teeth. They can also close gaps, lengthen short teeth, or permanently brighten discolored teeth.
Porcelain has been traditionally chosen for the job because it looks natural, transmits light beautifully, and has excellent color stability. The life expectancy is also good, with many veneers lasting up to fifteen years. Unfortunately, at $1,000 to $2,500 per tooth, they can also be rather expensive.
Nevertheless, apart from the cost, their many advantages have made them a popular choice. There are several disadvantages, however. Among these is that most porcelain veneer procedures are irreversible. This means that the slight amount of tooth reduction necessary to create a natural appearance commits the patient to future veneers. Also, in most cases, multiple visits are required – with anesthesia. And should a veneer ever become damaged, or should it break, it is not easily repaired. It typically requires replacement.
Fortunately, an alternative form of treatment exists. As long as the dentist does not have to restore tooth decay as well, it can generally be performed without anesthesia.
This is known as a direct composite resin veneer. Instead of using porcelain to cover the tooth, a dentist places a very thin layer of composite resin – essentially, a tooth-colored filling material – over the tooth in order to create a similar effect. Whereas in the past, this solution sometimes resulted in a dull, lifeless appearance for a tooth, current composite resins available to dentists have improved significantly. Products on the market today have enhanced physical and optical properties that also allow the dentist to accomplish a dramatic change in a patient’s appearance in as little as one visit. Many composite resins can also be placed with little or no alteration of the tooth’s structure. Every person’s case is different, however. Your dentist should be able to give you an idea of what will be required to obtain the optimal esthetic result for your case. Expect to pay anywhere between $350 to $695 per tooth.
What if you break or chip a composite resin veneer? The repair is usually easy to accomplish in a single visit and at a significantly reduced cost to replacing a porcelain veneer. Are there any disadvantages? Frankly, these are among the most technique sensitive of all dental veneers. The skill of the dentist and their attention to detail are critical elements in achieving a good result.
Talk with your doctor about which options are right for you. It may still be possible for you to enjoy the benefit of veneers – at nearly half the cost. Most dental offices today offer flexible financing options, many of which are interest free. Your perfect smile may be much closer than you think!
Dr. Richard Walicki is a dentist practicing general and cosmetic dentistry. While we hope you find the information contained herein interesting and useful, this blog is for informational purposes and is not intended to diagnose any oral disease. Dental conditions should be evaluated by your dental health professional or a qualified specialist.
Search by Topic
Get Access To The AWESOME Health Course
In this 12 week program, you’re going to discover how to achieve AWESOME health and double your energy with natural, tested, and scientific strategies. Just click on the image below: