When we are born we come into the world without teeth. Some of us leave the same way, but that really isn’t what nature intended.
When you are on a liquid diet having teeth doesn’t appear to be vital, since there is obviously nothing to chew. Nature pretty much handles a baby’s nutritional needs with mother’s milk. As we grow and begin to eat solid food, however, having and maintaining healthy teeth becomes an entirely different matter.
So when teeth become lost due to cavities, periodontal disease or trauma, the consequences for good health can become significant. Let’s not forget that digestion begins in the mouth. There are actually two forms of digestion – mechanical and chemical.
Mechanical digestion is the grinding and tearing of food, as in chewing, in order to increase its surface area. Creating a greater surface area means that there is a better chance that chemical digestion can do its job. In chemical digestion, enzymes react with the food to help break it down into simpler substances which can either be absorbed in the bloodstream as nutrients or passed out of the body as waste. This process of breakdown and assimilation occurs within the digestive tract – but it starts in the mouth with your teeth, tongue, and saliva.
Because a full set of adult teeth numbers thirty-two, it seems many people feel the occasional loss of a tooth is a relatively insignificant event. And while it is true that a person can still function with thirty-one, the long-term consequence of losing just one tooth can be more significant than most people realize.
While all of our teeth are important, structurally, the loss of certain teeth will bring about more change than the loss of others. Think of this in terms of the walls of your house. If you take down a non-supporting wall, the house will still stand. Take out a supporting wall, however, and you have a much bigger problem. Teeth are constructed much like an arch, though. If you have ever seen a stone arch, you know it has a keystone at the top that keeps the arch together. Remove that one stone, and the whole thing collapses. In your dental arch, you can think of your canines as a keystone. Lose them, and the ensuing change can be rapid. You can lose several teeth – even all – over time. But it’s not just the loss of canines that creates a problem.
Losing a first molar, for example, can create a domino effect of changes in your mouth that can affect your ability to chew easily. It can cause shifting of the teeth in a manner that even affects the appearance of your front teeth. Or, it can lead to periodontal problems and the formation of cavities on portions of the teeth that might not have been otherwise affected before the loss.
The point is that if you lose a tooth, you should consult your dentist about what tooth replacement options are right for you. Today, we have many ways of providing functional replacements that can improve your ability to chew your food, maintain your good appearance, and keep you from losing still more teeth. Depending upon your circumstances and financial considerations, these replacements may include removable dentures, bridges (which are non-removable, cemented tooth replacements), or dental implants (think of them as artificial tooth-roots that have crowns, bridges, or dentures attached to them).
If you are missing a tooth, speak with your dentist about what tooth replacement options are right for your situation. Replacing a lost tooth early is often much less involved (and costly) than when you begin to experience the problems resulting from long-term neglect.
Years of practice have convinced me that most people don’t “get” this — but they should.
Here’s how I know, and why you need to understand periodontal disease.
Now, when I say people don’t “get” periodontal disease, what I mean is that they don’t understand it. Naturally, the problem is that they do get it, and in much larger numbers than was previously considered to be the case.
According to recent findings from the Centers for Disease Control and Prevention (CDC) and the American Academy of Periodontology, nearly half of American adults older than age 30 years have periodontal disease. These studies also found that the prevalence of periodontitis rises to 70.1% in adults older than age 65.
Study authors found that 47.2% of the population (which would account for approximately 64.7 million adults) has periodontal disease, a figure far higher than previous national estimates.
So how do I know most people don’t understand the problem?
Here are two real-life examples that I encounter much too often:
Scenario One:
When told they have periodontal disease, the patient responds — “Oh, yeah. I had that treated once some years ago.”
Scenario Two:
Dentist: You have periodontal disease.
Patient: Yes, my last dentist told me and I got the treatment.
Dentist: Do you understand what it is?
Patient: No.
The last scenario is an obvious case of non-understanding, by the patient’s very admission. (This was an actual exchange, by the way.) But what is it about the first one that lets me know the person doesn’t really understand their condition? Simply this:
If not controlled, periodontal disease can be progressive. If controlled once, but later neglected, it can return. Usually, at this point in the discussion, it has returned and the patient is not aware of it. Its not like a childhood disease that you get once and then never again.
In fact, there is a reason it is the number one cause of tooth loss worldwide and it is that most people just don’t know they have it. In a great many cases — probably most — it doesn’t hurt until it is too late.
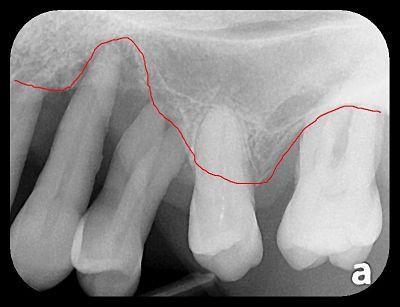
Take a look at the x-ray to the left:
The red line roughly traces the patient’s bone level.
Would you expect this patient’s teeth to be loose?
If you answered “yes” you would be correct. There is little there to support them.
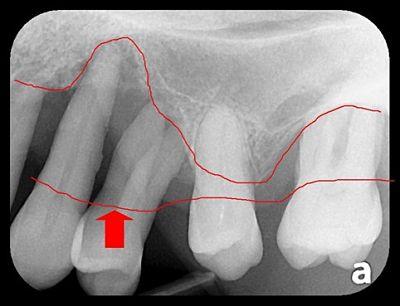
Now look at the second x-ray:
Notice the lower line marked by the red arrow.
This is approximately where the patient’s bone used to be.
That’s periodontal disease.
(It is also sometimes called “gum disease” because the gums that lay over the bone are generaly affected as well.)
Sometimes, it is not until I trace these lines out for people that they really get it. I hope you understand it a little better now, too, because there is a very good chance you may have it or get it at some point in your life — and it probably won’t give you much of a warning sign in the early stages.
Periodontal disease doesn’t have to be evenly distributed in the mouth. It can limited to one or several teeth. Everybody has a different predisposition to periodontal disease, but there is a great deal you can do to prevent it.
Step one is see your dentist for an examination if you haven’t had one in a while. Ask questions and learn more about what you can do to halt its spread. Wouldn’t you rather be in the group of 30% that doesn’t have periodontal disease than the group of 70% that do?
Do you suffer from a loose lower denture or have a family member who is having a rough time wearing their denture?
Unfortunately, this is a common problem. When all of the lower teeth are missing, little remains to stabilize or retain the denture.
An upper denture actually creates some suction on the roof of the mouth and will generally hold well. Not so, with the lower denture. First of all, the tongue has a tendency to displace it and because the surface area that the denture rests upon is generally narrow – there is little surface tension to hold it in place.
Many denture wearers have to rely on adhesives to keep their dentures from flopping around while they speak or eat. In a number of cases, even these adhesives fall short of their objective. Not to mention the fact that many patients find the adhesives unpalatable and some concerns have been recently raised about zinc sensitivities and copper de
ficiencies associated with these products.
Eating with full lower dentures can become difficult or even painful. Patients often opt not to wear their lower dentures at all out of frustration or embarrassment. Unfortunately, this can make it difficult to eat certain foods that are needed for good nutrition and health.
Numerous remedies have been forwarded to solve the problem in addition to adhesives. For example, relines can create an improved fit but they still don’t overcome the inherent problems described above. Then, there are dentures that are designed to look like they have octopus suction cups on the bottom, dentures with valves to suck out the air that gets under them, and dentures that have little “wings” on them that hold the denture down by the weight of the tongue.
Probably the greatest advance in denture stability, however, has been the development of dental implants. If a person has enough bone that is of good quality (not too soft) to accept implants, little comes close to these to provide both retention and stability for a loose lower denture. Also, much of the pain associated with dentures moving around and creating sore gums is eliminated because the denture is actually supported by the implants.
But what if you have been told you are not a candidate for conventional implants because of insufficient bone? Countless patients have still been able to benefit from mini-implants.
These are extremely small (1.8 mm diameter) implants that can be used for critically needed support purposes. Mini-implants can and do serve as long-term devices. In fact, some have been successfully functioning in patients for decades.
Because they are so narrow, they can typically be inserted directly through the overlying gum tissue into the bone underneath. This means that the procedure is generally much more comfortable for the patient because (in most cases) there is no need to surgically cut open the gum tissue – routinely required for standard implant cases. As a result, post-operative patient irritation and soreness is significantly reduced.
It should be mentioned that no implant system is fool-proof or has any guarantee of longevity. Such factors as poor oral hygiene, poor health, stress-inducing habits such as tooth grinding and clenching, smoking, poor health, osteoporosis, medications, and lack of follow-up care can all lead to potential failure of the implants. Compared to conventional implants, however, the cost of replacement is generally much smaller and with less bone loss and gum deterioration. Failures involving mini-implants are not unheard of, but are generally quite rare.
As you might expect fees vary from doctor to doctor and by geographic location. Generally, though, the fees tend to be a lot lower than for conventional implants – with similar results, less discomfort and much shorter waiting times. The best way to address the cost issue is to have an open and honest discussion about what fees may arise with the dentist of your choice.
Many dentists now consider an implant-stabilized lower denture the new “standard of care.” By choosing this option you are deciding upon an improved way of life that is free of so many of the heartaches and discomforts associated with loose, painful and ill-fitting dentures. Because people need to use their teeth each and every day of their lives, that’s worth a great deal.
When many people think of a dentist, one of the first associations they make has to do with filling cavities. While this has traditionally been one thing dentists are known for, it is far from the complete picture.
Nevertheless, tooth decay is one of the most common diseases world-wide and, if neglected, can become one of the most expensive to treat. Our practice philosphy is that it is far better to prevent a problem from occurring than it is to treat it. For that reason, we feel it is important for you to understand your condition so that you can make informed decisions.
If knowledge is power, then we want you to be able to take control of your dental health with useful and practical information.
After over twenty years of practice I have learned that many patients feel a cavity should hurt before you treat it.. Unfortunately, that can be a formula for disaster. Some time ago, I prepared this short video to explain just why that is.
Consider this article a public service announcement. I really dislike it when patients lose their teeth unnecessarily. My practice philosophy is that if a person has a dental problem, the goal is to handle that difficulty first, but then empower the patient with the correct knowledge that will keep him out of trouble from there on out. Ideally, my hope is that most future visits to my office will only be for routine maintenance.
Unfortunately, and all too often, I encounter new patients with teeth that are so badly decayed there is little hope of salvage. Possibly just as frequently, I find these patients scheduling a checkup – usually after a long absence from dental care – who are surprised to learn that they have any cavities at all. Sometimes they will think they lost a filling when, in fact, a piece of their enamel has broken away.
Why are they surprised? The common denominator seems to be the idea that cavities are supposed to hurt.
Well, sometimes they do hurt. But most of the time – especially in the early stage – they don’t.
In fact, by the time a tooth does start to hurt you it’s usually pretty bad. More often than not, it is so bad that a dentist is evaluating whether it can be treated with endodontic (root canal) therapy or whether it needs to be extracted. A little understanding of basic dental anatomy is helpful here.
Take a look at the illustration below:
The outer layer of the tooth is comprised of enamel. This is the hardest substance in your body. It breaks up your food and is designed to last you a lifetime.
And now, here is the important part for you to understand: it doesn’t contain any nerves.
It is more than ninety-five percent mineral. Water and organic materials make up the balance. And because it doesn’t have nerves, it doesn’t have feeling. This is actually quite practical since it wouldn’t do to have pain every time you bit into something. On the other hand, it also means that it can be decayed without giving you a warning.
In fact, decay can also travel into the supporting layer – the dentin – and still not cause you pain. It usually has to travel pretty close to the inner layer that contains the blood vessels and nerves – the pulp – before you feel it. Of course, by then, the tooth has generally undergone considerable destruction.
Another factor that makes spotting decay difficult is the way it spreads. I have drawn two black triangles into the enamel above. Notice that the narrow point is on the outside of the enamel. The broader base faces the inside of the tooth. This is how decay usually travels. Sometimes, it will undermine the interior of the tooth while the outer, harder enamel still maintains its form . . . until it eventually crumbles because the underlying supporting dentin has been eaten away by decay.
Many cavities also form at the contact point between two teeth. These are areas that you simply cannot see. Even the dentist needs an x-ray to spot these cavities in most cases.
So what does all this really mean? Spotting decay is not always that easy. As dentists, we use visual examination, but we also rely on probes, x-rays, and even laser detection devices to locate cavities. Even then, it can be difficult to find cavities under existing fillings.
Don’t rely on pain to tell you if you have a cavity in your tooth. If you do, you can be assured that your treatment is likely to be more uncomfortable, expensive, and may even result in the loss of a tooth that could have been treated much more easily earlier in the game.
If you have a loved one, who still has their teeth and hasn’t seen a dentist in a while, have them read this article. You may be saving them from quite a bit of discomfort – not to mention time and money – if they catch potential problems before they are hopeless.
Some of you may be thinking, “No big deal. If it’s that bad, I’ll just pull it.” OK, sometimes that is necessary, but therein lies a lesson for another day.
While I believe you can find many useful tips on this site to help you improve your dental health, if there were only ONE thing I might impart to you that may help you achieve a more desirable oral condition – it would be to gain an understanding of the role your diet plays in the formation of tooth decay.
Over the years I have seen patients with good oral hygiene experience little decay and patients with poor oral hygiene experience the same. Conversely, I have seen several patients with excellent hygiene still experience problems with tooth decay. And of course, there are those patients with poor oral hygiene who, as one might expect, experience difficulties. Maybe it is all a matter of your genes, then?
If so, what about my genetically identical patients (twins)? One has virtually no tooth decay, whereas, the other has had a cavity in almost every other tooth in her mouth.
The difference, in virtually all of these cases is diet.
Patients with a tooth-friendly diet experience less decay than those who consume foods that are not good for your teeth. And, frankly, a tooth friendly diet is a body-friendly diet. So this begs the question: is tooth decay a problem of bacteria, or diet?
I believe both play their role. But you can control your diet and, to that degree, what you eat is most likely the very key to your dental health. Click on the links above to read about foods that are good for your teeth and those that are not.
Cosmetic dentistry isn’t always just about good looks. Many of these treatments can improve various oral problems, such as correcting your bite. They are also not necessarily restricted to the teeth. Some people encounter problems with gum pigmentation or uneven gums. Periodontal procedures exist that address these difficulties as well.
Generally, cosmetic dental procedures include whitening, bonding, crowns, veneers, and the reshaping and contouring of teeth. If you have a cosmetic concern, it is a good idea to have heart-to-heart talk with your dentist and ask lots of questions. Among them:
What can I expect the changes will look like?
What should I experience throughout the course of treatment?
What type of maintenance will be required by me or by the dentist?
Television has certainly popularized cosmetic dentistry with such shows as Extreme Makeover and, at times, it can be as complex as a total smile reconstruction. At other times, cosmetic dentistry may be as simple as correcting the appearance of a single tooth. In short, it is what is right for you, what fits your budget, and makes you feel better about your smile!
Dr. Richard Walicki is a dentist practicing general and cosmetic dentistry. While we hope you find the information contained herein interesting and useful, this blog is for informational purposes and is not intended to diagnose any oral disease. Dental conditions should be evaluated by your dental health professional or a qualified specialist.
Search by Topic
Get Access To The AWESOME Health Course
In this 12 week program, you’re going to discover how to achieve AWESOME health and double your energy with natural, tested, and scientific strategies. Just click on the image below:
 So when teeth become lost due to cavities, periodontal disease or trauma, the consequences for good health can become significant. Let’s not forget that digestion begins in the mouth. There are actually two forms of digestion – mechanical and chemical.
So when teeth become lost due to cavities, periodontal disease or trauma, the consequences for good health can become significant. Let’s not forget that digestion begins in the mouth. There are actually two forms of digestion – mechanical and chemical.