What?! Is the sky falling? What dentist would dare utter such blasphemy!
Stick with me for a moment. You may learn something about flossing.
Here are the facts as I see them after more than twenty years in dental practice:
Most patients don’t floss. Most patients don’t like to floss. Most patients won’t floss even if you explain the benefits of flossing at every checkup visit for ten years. Most patients are convinced flossing makes their gums bleed and is uncomfortable to do. Most patients will tell you they floss, but “probably not as much as I should.” So really, why bother?
Another observation I have made about flossing regards what people think flossing is. I will sometimes hand a patient a piece of floss and ask them to show me how they floss. Without exception, I have seen patients pass the floss between their teeth and then pop it back out.
That sounds right, doesn’t it? Special effects department please sound the buzzer. That’s not flossing.
Add to this the fact that most patients will only perform this routine once in a while. If you call that “flossing” I say don’t lose sleep over the fact that you are not flossing regularly. That can be effective at pulling food out from in between your teeth, though, so feel free to do so. But if that’s not flossing, just what is it, really?
Flossing is the action of taking a length of floss – either the conventional “string” kind or pre-threaded on a fork-like device – and then passing it between your teeth while holding it in a “C-shape” against the side of the tooth. You then take the floss and rub the edge of the tooth, sliding it all the way under the gum-line in an up and down motion. How often can one do this? After every meal would not be too much. But if people did this at least once a day, the average case would see dramatic results after an average of two weeks of daily flossing.
If you haven’t been flossing regularly here is what you can expect: your gums will bleed when you start to floss. It is also likely to be a little uncomfortable at first. But over time, the bleeding should stop. If you haven’t had a dental checkup and cleaning for a while, it is a good idea to do so this first. Flossing against existing tartar will be an unending battle. Once the teeth are clean, however, daily flossing will usually result in pink, firm and healthy gums that don’t bleed. Other benefits? Fresher breath and reduced inflammation – which also means a lowered chance of heart attack and stroke.
If you only floss once in a while, though, inflamed gums will likely never get up to a point where the occasional activity makes any difference. So, if you don’t make it a discipline, why bother? But if you would like healthy teeth and gums for a lifetime, start flossing today!
There are a number of factors that can contribute to the formation of dental cavities. One fundamental that will apply to most everyone concerns the reduction of dental plaque. If you want fewer cavities, reduce your plaque levels.
Dental plaque can be defined as a complex microbial community, with greater than 10 to the 10th power bacteria per milligram. (That’s really a lot of bacteria.) Just to keep things simple, though, the problem is that these bacteria produce acids on your teeth – and the acids dissolve the enamel, leading to tooth decay.
After only a few years of practice, it became obvious to me that most people have difficulty identifying plaque. Even now, I’ll begin a dental exam or cleaning on a person and start removing large areas of plaque. If I casually ask the patient about their cleaning regimen, often I’m told “I brushed just before I came in here!”
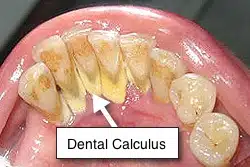
Since that much plaque can’t form in an hour, the obvious conclusion is that the patient missed it or simply doesn’t see it. Just to be clear, plaque is the soft, sticky film that occurs on the surface of teeth – not the hard substance your dentist or hygienist has to pick away, which is tartar. Though it is basically mineralized plaque, virtually no amount of tooth brushing and flossing will remove tartar after the fact (dentists call it ‘calculus’). Once formed, calculus needs to be removed at your office visit.
It is useful to know that if you control your plaque well, calculus won’t be much of a problem. So let’s focus on that for a moment. What do you do if you feel you are brushing, but the dentist tells you he still sees plaque? Stain it!
Lately, I have been seeing more commercials advertising products for children that stain their teeth blue after they have rinsed with it. The child then brushes until all of the blue stain has been removed. What the liquid is staining is plaque. I think this is a great way to simplify the process of identifying the problem. Whether you are six or sixty, the principle is the same.
If you want to be certain you have gotten the plaque off, rinse with the stain after each meal and then brush (and floss) until you have removed the discolored areas. Barring other systemic or external contributory factors (such as medications leading to a dry mouth), you and your dentist should see a big improvement in the cleanliness of your mouth, and fewer cavities over time!
When we are born we come into the world without teeth. Some of us leave the same way, but that really isn’t what nature intended.
When you are on a liquid diet having teeth doesn’t appear to be vital, since there is obviously nothing to chew. Nature pretty much handles a baby’s nutritional needs with mother’s milk. As we grow and begin to eat solid food, however, having and maintaining healthy teeth becomes an entirely different matter.
So when teeth become lost due to cavities, periodontal disease or trauma, the consequences for good health can become significant. Let’s not forget that digestion begins in the mouth. There are actually two forms of digestion – mechanical and chemical.
Mechanical digestion is the grinding and tearing of food, as in chewing, in order to increase its surface area. Creating a greater surface area means that there is a better chance that chemical digestion can do its job. In chemical digestion, enzymes react with the food to help break it down into simpler substances which can either be absorbed in the bloodstream as nutrients or passed out of the body as waste. This process of breakdown and assimilation occurs within the digestive tract – but it starts in the mouth with your teeth, tongue, and saliva.
Because a full set of adult teeth numbers thirty-two, it seems many people feel the occasional loss of a tooth is a relatively insignificant event. And while it is true that a person can still function with thirty-one, the long-term consequence of losing just one tooth can be more significant than most people realize.
While all of our teeth are important, structurally, the loss of certain teeth will bring about more change than the loss of others. Think of this in terms of the walls of your house. If you take down a non-supporting wall, the house will still stand. Take out a supporting wall, however, and you have a much bigger problem. Teeth are constructed much like an arch, though. If you have ever seen a stone arch, you know it has a keystone at the top that keeps the arch together. Remove that one stone, and the whole thing collapses. In your dental arch, you can think of your canines as a keystone. Lose them, and the ensuing change can be rapid. You can lose several teeth – even all – over time. But it’s not just the loss of canines that creates a problem.
Losing a first molar, for example, can create a domino effect of changes in your mouth that can affect your ability to chew easily. It can cause shifting of the teeth in a manner that even affects the appearance of your front teeth. Or, it can lead to periodontal problems and the formation of cavities on portions of the teeth that might not have been otherwise affected before the loss.
The point is that if you lose a tooth, you should consult your dentist about what tooth replacement options are right for you. Today, we have many ways of providing functional replacements that can improve your ability to chew your food, maintain your good appearance, and keep you from losing still more teeth. Depending upon your circumstances and financial considerations, these replacements may include removable dentures, bridges (which are non-removable, cemented tooth replacements), or dental implants (think of them as artificial tooth-roots that have crowns, bridges, or dentures attached to them).
If you are missing a tooth, speak with your dentist about what tooth replacement options are right for your situation. Replacing a lost tooth early is often much less involved (and costly) than when you begin to experience the problems resulting from long-term neglect.
Dry mouth, also called xerostomia, is a common oral health problem. Unfortunately, for some patients it becomes a “silent” condition that often goes undiagnosed and untreated. While there are many potential reasons for this condition, one of the most frequent contributing factors is the use of medications. Over four hundred commonly prescribed drugs list dry mouth as a potential side effect.
While this condition is fairly common in the general population, the prevalence increases with age. This is likely because many older adults take medications for one or a number of co-existing medical conditions.
Though some people may consider dry mouth an inconsequential medical or dental concern, it can be a troublesome symptom also associated with systemic diseases and health conditions. Things that most people take for granted, such as being able to chew their food – or even to taste it – result in a reduced quality of life for the patient with xerostomia.
Negative effects of dry mouth can include:
• Increased dental decay
• Oral infections
• Cracks and fissures in the tissues of the mouth
• Denture sores and ulcerations
• A decreased willingness or ability to speak easily
Keep in mind that almost everyone has experienced dry mouth at some time in their lives. Dehydration following excessive perspiration, diarrhea, or alcohol consumption are experiences many people have experienced at one time or another. These situations are generally transient and easily identified. It should be noted here that not only alcohol consumption, but simply rinsing with alcohol-containing mouthwashes can result in a dry mouth. Many patients hold these rinses in their mouths for much longer than the recommended 30 second period. This can produce a type of tissue burn called sloughing; however, even regular use can cause a drying effect for many individuals.
If, however, you find any of the following problems to be daily events, you should raise the issue with your dentist or physician:
• Do you consistently need to sip liquids to help you to swallow your food?
• Does your mouth feel dry whenever you eat?
• Do you have any difficulty swallowing?
• Does the amount of saliva in your mouth seem to be much less than you remember, or do you not notice the difference?
There are several simple things your health practitioner can do to evaluate your condition. A medical history will also provide clues. For example, certain conditions such as diabetes, cancer treatments, and Sjögren’s syndrome have also been connected with dry mouth. (Sjögren’s syndrome is a chronic autoimmune disease in which a person’s white blood cells attack their moisture-producing glands.)
Keep in mind that dry mouth symptoms may not appear until saliva production has been reduced to approximately half the normal flow.
While it is always best to identify the source of the problem to seek a long-term resolution, sometimes it is necessary to provide symptomatic relief. A number of products have been developed that can help the dry-mouth patient who so often has extra sensitive mouth tissues. These include stimulation products such as chewing gums, specially formulated toothpastes and mouthwashes that are free of irritating ingredients, and moisturizing gels or sprays.
The important thing is that you do not ignore dry mouth symptoms if they exist. Talk to your dentist or doctor. Day-to-day symptoms and their complications can be managed. If you and your doctor correctly identify the source, perhaps those problems can even be eliminated over time. The simple pleasures of life – eating comfortably, tasting an enjoyable meal, laughing freely – shouldn’t be just a memory.
If you require that a cosmetic dental crown be placed, it is a good idea to evaluate how you feel about the color of your existing teeth before the process is initiated. If you like the color of your teeth, the dentist will then find a crown shade that matches them.
On the other hand, if you feel that you would like your teeth to be lighter, bleaching may be an option for you. If you know you would like to whiten or lighten the shade of your teeth, it is a good idea to communicate this to the doctor beforehand. Once the final crown or cosmetic restorations are made, it will not be possible to change their color without re-doing them.
While bleaching is generally predictable, the results do not last forever. You may have to touch them up every one to three years. Teeth will re-darken. (This tends to occur more slowly with Power Bleaching.) The rate at which it happens, though, depends upon your habits. The good news is that your teeth can be brightened once again. Just remember, crowns and fillings do not change their color with bleaching — only your natural teeth will lighten.
Dr. Richard Walicki is a dentist practicing general and cosmetic dentistry. While we hope you find the information contained herein interesting and useful, this blog is for informational purposes and is not intended to diagnose any oral disease. Dental conditions should be evaluated by your dental health professional or a qualified specialist.
Search by Topic
Get Access To The AWESOME Health Course
In this 12 week program, you’re going to discover how to achieve AWESOME health and double your energy with natural, tested, and scientific strategies. Just click on the image below: