How long do fillings last? It is one of the most common—and most reasonable—questions patients ask. The honest answer is that dental restorations do not come with a guaranteed expiration date. Some fillings and crowns last only a few years, while others serve beautifully for decades.
So when people ask how long do fillings last, what they are really asking is how long they can expect their dental work to hold up under real-life conditions.
The difference often comes down to the size of the restoration, where it is in the mouth, the patient’s bite, oral hygiene, diet, habits such as clenching or grinding, and the material used.
How Long Do Fillings Last? 7 Key Factors That Make the Difference
Many insurance guidelines and dental studies place the average life of fillings and other restorations somewhere around five to seven years. That does not mean every filling fails at that point. It means that, across large groups of people with very different mouths and habits, that range is often used as a practical benchmark.
This helps explain why the answer to “how long do fillings last” can vary so widely from one person to another.
In real-world dentistry, the range is much wider. A small filling in a low-stress area may last many years. A large filling on a heavily used back tooth may have a much shorter life, especially if the patient clenches or grinds.
For readers who want a general overview of filling materials, the American Dental Association has a helpful guide to dental filling options.
1. Small Fillings Usually Last Longer Than Large Fillings
One of the most important factors is the amount of natural tooth left to support the restoration.
A small filling placed in a small cavity usually has strong tooth structure around it. That support helps the filling hold up over time. A large filling is different. When more tooth structure has been lost, the remaining tooth is weaker, and the restoration has to carry more of the chewing load.
That is why a large filling may eventually need to be replaced with a crown. The issue is not always that the filling material “went bad.” Often, the tooth simply no longer has enough strength to keep functioning the same way.
2. Back Teeth Take More Abuse
Location matters, too.
Back teeth handle most of the heavy chewing force. Molars, especially, take tremendous pressure every day. A filling or crown on a back tooth is working in a much harsher environment than a small repair on a front tooth.
This is one reason two people can receive similar restorations and have very different outcomes. The tooth, the bite, and the forces placed on that restoration all matter.
3. Bruxism Can Shorten the Life of Fillings and Crowns
Bruxism—clenching or grinding the teeth—is one of the biggest reasons restorations fail earlier than expected. A person who grinds heavily is simply not putting the same level of stress on dental work as someone who does not.
Over the years, bruxism has become much more common. Earlier in my career, it was something we saw occasionally. Today, it is something dentists see almost every day.
Clenching and grinding can crack fillings, chip porcelain, loosen crowns, fracture teeth, and even place excessive stress on implants. Night guards can help protect the teeth, but only when they are worn consistently.
This is one of the biggest reasons how long fillings last differs so much between patients.
4. Material Choice Matters, But It Is Not the Whole Story
The material used for a filling or crown can affect longevity. Some crown materials are more prone to chipping in heavy grinders. Others, such as solid zirconia, are extremely strong.
But stronger is not always automatically better. In a severe grinder, a very strong crown may survive while the tooth or root beneath it absorbs the stress. In other words, the restoration may not break—but something else can.
This is why material choice should be personalized. The best option depends on the tooth, the bite, the patient’s habits, esthetics, and long-term risk.
5. Diet and Oral Hygiene Affect How Long Fillings Last
Sometimes a restoration fails because of wear or fracture. Other times, the problem is new decay forming around the edges.
A clean mouth gives fillings and crowns a much better chance of lasting. Frequent sugar exposure, acidic drinks, constant snacking, and poor brushing or flossing can all shorten the life of dental work.
When decay forms around an existing filling or crown, the restoration may need to be replaced even if the material itself is still intact.
6. Cracked Teeth Can Change the Timeline
A tooth with cracks is less predictable. Even a well-made filling or crown may have a shorter lifespan if the tooth underneath has already been weakened.
Cracks may develop from old large fillings, heavy bite forces, trauma, or years of grinding. If you have symptoms such as sharp pain when biting, sensitivity, or discomfort that comes and goes, this ToothWiz article on a cracked tooth may be helpful.
7. Home Care and Regular Dental Visits Help Restorations Last
One of the best ways to improve the lifespan of dental work is to find problems early. A small chip, open margin, bite issue, or area of early decay may be manageable if caught soon enough.
Regular dental visits allow your dentist to monitor old fillings and crowns before they become bigger problems. Good brushing, flossing, and limiting frequent sugar exposure also help create the kind of oral environment where restorations can last longer.
So, How Long Should You Expect a Filling or Crown to Last?
By this point, it should be clear that how long do fillings last depends on far more than just the material used.
A fair answer is this: many restorations last around five to seven years on average, but many last much longer. Ten, fifteen, twenty years or more is possible when the tooth is well-supported, the bite is stable, the mouth is clean, and destructive habits are controlled.
The better question may be: What can we do to help this restoration last as long as possible?
That means choosing the right material, keeping the mouth clean, reducing sugar and acid exposure, watching for signs of grinding, wearing a night guard when recommended, and having restorations checked regularly.
The Bottom Line on How Long Fillings Last
How long do fillings last? The answer depends on the person, the tooth, and the conditions in the mouth. A small filling in a healthy, low-stress environment may last for decades. A larger restoration under heavy load may need attention much sooner.
Dental work lasts longest when it is supported by healthy tooth structure, good home care, smart material choices, and a bite that is not constantly overloading it.
Frequently Asked Questions
Do fillings last forever?
No. Even the best fillings wear down over time, although some can last for decades with proper care.
How do I know if my filling needs to be replaced?
Signs include sensitivity, rough edges, pain when biting, or visible cracks. Regular dental exams help catch problems early.
Sugar and vitamin C absorption is a topic that deserves more attention—especially when it comes to your gum health. While sugar does not completely block vitamin C from entering your body, it can interfere with how effectively your cells absorb and use it, particularly when blood sugar levels are elevated.
This interaction is subtle, but clinically important. It helps explain why some patients experience persistent gum inflammation even when their diet appears adequate in vitamin C.
How Sugar and Vitamin C Absorption Work in the Body
To understand the relationship between sugar and vitamin C absorption, we need to separate two processes: absorption from the gut and uptake into your cells.
Intestinal Absorption Is Mostly Unaffected
Vitamin C (ascorbic acid) is absorbed in the small intestine through sodium-dependent transporters (SVCT1). These transporters are different from glucose pathways, so sugar does not significantly block vitamin C at the digestive level.
This means your body can still absorb vitamin C even if sugar is present in the diet.
Cellular Uptake Is Where Sugar Competes
The more important interaction happens after absorption.
Vitamin C also exists as dehydroascorbic acid (DHAA), which uses glucose transporters (GLUTs) to enter cells. Because DHAA closely resembles glucose, elevated blood sugar can compete with and reduce its uptake.
Research has shown that glucose can inhibit vitamin C uptake into cells in a concentration-dependent manner (PubMed study).
Additional biochemical evidence supports this competitive relationship between glucose and vitamin C transport (ScienceDirect research).
In practical terms, higher blood sugar levels may mean less vitamin C gets into your cells—where it’s actually needed.
Why Sugar and Vitamin C Absorption Matter for Gum Health
The connection between sugar and vitamin C absorption becomes especially important when we look at oral health.
Vitamin C Supports Gum Structure and Healing
Vitamin C is essential for collagen production, which forms the structural foundation of your gums and periodontal ligaments. It also plays a key role in reducing inflammation and supporting immune function.
When vitamin C levels inside cells are reduced, you may begin to see:
Bleeding gums
Swelling or tenderness
Delayed healing after dental work
Increased risk of periodontal disease
Clinical evidence suggests that improving vitamin C intake can help reduce gingival bleeding and inflammation (clinical overview).
This combination weakens gum tissue while increasing bacterial damage—an ideal setup for periodontal breakdown.
Does Timing Affect Sugar and Vitamin C Absorption?
Timing likely plays a role in optimizing sugar and vitamin C absorption at the cellular level.
Because glucose competes with vitamin C transport, taking vitamin C when blood sugar is lower may improve tissue uptake.
Simple strategies include:
Taking vitamin C supplements away from high-sugar meals
Avoiding sugary drinks when supplementing
Spacing intake throughout the day
Whole food sources of vitamin C also tend to produce a slower blood sugar response, which may reduce this competition.
Choosing a Tooth-Friendly Vitamin C Option
Avoid Sugary and Acidic Forms
Chewable tablets and vitamin C gummies often combine sugar and acidity—two factors that can damage enamel over time.
Consider Liposomal Vitamin C
Liposomal vitamin C may offer better absorption and reduced contact with teeth. It encapsulates vitamin C in lipid layers, potentially improving delivery into cells.
When we step back, the relationship between sugar and vitamin C absorption helps explain a common clinical pattern: higher sugar intake often correlates with more gum inflammation—even when vitamin intake seems adequate.
This effect may be even more pronounced in individuals with frequent blood sugar spikes or diabetes.
Understand that absorption and utilization are different
Time vitamin C intake away from high-sugar meals
Choose tooth-friendly supplement forms
Maintain consistent oral hygiene and dental care
Final Thoughts on Sugar and Vitamin C Absorption
The science behind sugar and vitamin C absorption shows that sugar doesn’t completely block vitamin C—but it can interfere with how effectively your body uses it.
For your gums, this can mean weaker collagen, more inflammation, and slower healing over time.
Managing sugar intake while supporting vitamin C status is a simple but powerful way to protect your oral health.
By Richard J. Walicki, DMD | toothwiz.comInterest in herbs for oral health has grown as more people look for natural ways to support gum health and fresh breath. Modern dentistry is excellent at treating problems like cavities and gum disease. But prevention still starts with daily habits—and nature can offer
helpful allies. Across many traditional systems, herbs have been used to support oral hygiene, soothe inflamed tissue, help control odor-causing bacteria,
and freshen breath. Today, emerging clinical research suggests that some botanicals may complement brushing, flossing, and professional care. Many people are now exploring herbs for oral health as a preventive complement to brushing, flossing, and professional dental care. Here’s the key idea: herbs for oral health can be supportive, but they aren’t magic. They require a little know-how to use safely and effectively.
Below are eight practical principles—rooted in both dental common sense and evidence-informed herbal guidance—to help you get benefits without unintended side effects.
Using Herbs for Oral Health: 8 Principles for Safe, Smart Use
1) Think “whole-mouth support,” not single-symptom fixes
Conventional care often targets a specific endpoint (plaque levels, pocket depth, a painful tooth). Plant-based approaches are frequently used more
holistically—aiming at underlying drivers such as inflammation, microbial imbalance, tissue irritation, or even dry mouth.
Two people can describe the same symptom—“my gums feel irritated”—yet have very different causes. One may need anti-inflammatory support (irritation from
aggressive brushing, mouth breathing, or an inflamed gumline). Another may benefit more from antimicrobial strategies (biofilm control, tongue hygiene,
or targeted rinses). The goal is prevention and balance, not chasing a single “miracle” ingredient.
2) Not all botanicals are the same strength: food herbs vs. remedies
For oral use, it helps to think in three practical categories:
Food herbs (daily): Generally gentle options like garlic, ginger, parsley, and peppermint used in meals or teas.
Gentle medicinal herbs (short-term): For example, chamomile tea as a soothing rinse, sage tea as a traditional antimicrobial rinse, or green tea as a supportive mouthwash.
Stronger remedies (use cautiously): Examples include diluted clove oil for temporary tooth discomfort, or concentrated turmeric pastes used briefly and carefully.
“More” isn’t always better. Once symptoms improve, it’s usually wise to taper back rather than using stronger approaches indefinitely.
3) Dosage, quality, and form matter (a lot)
Botanicals are not standardized like prescription medications. Two products labeled the same can differ in potency and purity.
Choose reputable brands and avoid products with unclear sourcing or questionable additives—especially anything you’ll place on oral tissues.
Also consider form:
Tea/rinse: Often gentler and easier to tolerate for sensitive mouths.
Gel/paste: More concentrated and sometimes more irritating—use for limited time.
Essential oil: Highly concentrated—generally requires dilution and extra caution.
A good rule: start low (diluted, short contact time, once daily) and increase only if tolerated.
4) “Natural” doesn’t automatically mean safe
A common misconception is that plant-based equals harmless. In reality, the mouth is delicate tissue. Some botanicals can cause burning, irritation,
allergic reactions, or problems when used too often or at too high a concentration.
Clove oil: Often used for short-term tooth discomfort, but undiluted or repeated use can irritate or burn tissue.
Turmeric/curcumin: Promising in studies for plaque and gingival inflammation support, yet can stain surfaces and may irritate some mouths if used too concentrated or too frequently.
Essential oils: Potent and more likely to irritate if used “straight.”
If you’re pregnant, immunocompromised, managing chronic conditions, or on medications (especially blood thinners), it’s smart to run your plan by a clinician.
Using herbs for oral health as a gentle mouth rinse is one of the safest ways to start.
5) Preparation changes the outcome (safety + effectiveness)
When using herbs for oral health, how you prepare a botanical can change how it behaves in the mouth. Choose the method that fits your goal and your tolerance.
Whole cloves + a dropper bottle (alt: “Clove oil used cautiously for temporary tooth discomfort”)
Turmeric powder or root (alt: “Turmeric/curcumin used for gum support in short-term routines”)
Green tea leaves or brewed cup (alt: “Green tea rinse as an adjunct to brushing and flossing”)
Peppermint sprigs (alt: “Peppermint tea as a gentle breath-freshening rinse”)
Gentle rinses (easy, low-risk starting point)
Green tea rinse: Rich in catechins; research has examined green tea mouthwash as an adjunct to mechanical plaque control. (Study link)
Chamomile tea rinse: A traditional soothing option for irritated gums (especially when the tissue feels “hot” or inflamed).
Sage tea rinse: Traditionally used for oral freshness and microbial support.
Peppermint tea rinse: Commonly used for breath freshening and a clean mouthfeel.
Topicals and pastes (more targeted, more caution)
Diluted clove oil: Use a tiny amount on a cotton swab and apply briefly to the affected area—avoid prolonged contact.
Turmeric paste: If you experiment, keep contact time short, rinse thoroughly, and avoid abrasive scrubbing (staining risk).
Chewing/fresh herbs (traditional practices)
Parsley or basil: Often used to reduce food odors after meals.
Traditional chewing sticks (e.g., neem): Used historically for mechanical cleaning and freshness (still, technique and hygiene matter).
Whatever you use, remember: rinses and botanicals should support your routine—not replace brushing, flossing, interdental cleaning, and professional evaluation.
6) Monitor for reactions and stop quickly if something feels “off”
If you notice burning, swelling, new sores, worsening bleeding, or increased sensitivity, stop immediately. Some people are sensitive to certain plant families
(for example, those with ragweed allergies can sometimes react to chamomile). When in doubt, choose a gentler approach or skip the herb entirely.
7) Interactions can be real—especially if you’re using multiple products
Many people stack: herbal rinses, essential oils, whitening products, prescription rinses, supplements, and medications. That combination can be unpredictable.
Keep a simple list of what you’re using and share it with your dentist—especially if you have gum disease risk factors like diabetes, dry mouth, or smoking history.
8) Choose credible sources (and know when herbs are the wrong tool)
Social media “DIY mouthwash” recipes often skip dosing, dilution, and safety guidance. Look for evidence-informed dental and herbal sources.
For example, curcumin mouthwash has been studied for anti-plaque and anti-gingivitis effects and has been compared to chlorhexidine in clinical research.
(PubMed link)
And just as important: botanicals are not a substitute for diagnosis. If you have bleeding gums, persistent bad breath, a toothache, swelling, loose teeth,
or sores that don’t resolve, you need a professional evaluation.
Practical “Safe Start” Routine (Simple, Conservative, and Dentist-Friendly)
Foundation first: Brush twice daily, clean between teeth daily, and don’t ignore the gumline.
Add one gentle rinse: Start with a mild tea rinse (e.g., green tea) once daily for 7–10 days.
Track your response: Less bleeding? Less irritation? Better breath? If it worsens, stop.
Reassess: If symptoms persist, treat that as a signal to check for plaque retention, gum disease, dry mouth, reflux, or other root causes.
Final Thoughts
Used wisely, herbs for oral health can be a helpful layer of prevention—especially when they support gum comfort, breath freshness, and a balanced oral environment.
But the foundation stays the same: consistent home care and regular professional checkups.
If you’d like to explore vetted wellness-support options beyond the spice cabinet, you can also browse my practitioner-grade dispensary resources here: ToothWizVitamins.
And for more curiosity-driven dental education, you can visit: Weird Dental Facts.
Disclaimer: This article is for educational purposes and is not medical advice. Talk with a dentist or qualified professional before using herbs, especially if you have medical conditions or take medications.
References (selected)
Curcumin mouthwashes and gingivitis/plaque research: PubMed record
For years, both dentists and patients have blamed toothbrush abrasion for those small notches that sometimes appear at the gumline. It seems logical—brush too hard, wear away the tooth. Simple.
But clinical experience and research have gradually told a different story. And once you see it, you can’t unsee it.
Those notches—often called abfractions—are far more likely to be caused by stress from clenching and grinding than by your toothbrush. (See related: Understanding Tooth Clenching and Grinding)
Rethinking Toothbrush Abrasion and Gumline Wear
The traditional explanation was straightforward: aggressive brushing, especially with a hard toothbrush, scrubs away enamel near the gumline. Many patients still believe this—and to be fair, it’s not entirely wrong.
Toothbrush abrasion can affect teeth. But what it tends to do is dull and roughen the surface, not carve out the sharply defined notches we often see in practice.
That distinction matters.
What Actually Causes These Notches?
Modern understanding points strongly toward mechanical stress—specifically, the forces generated during clenching and grinding.
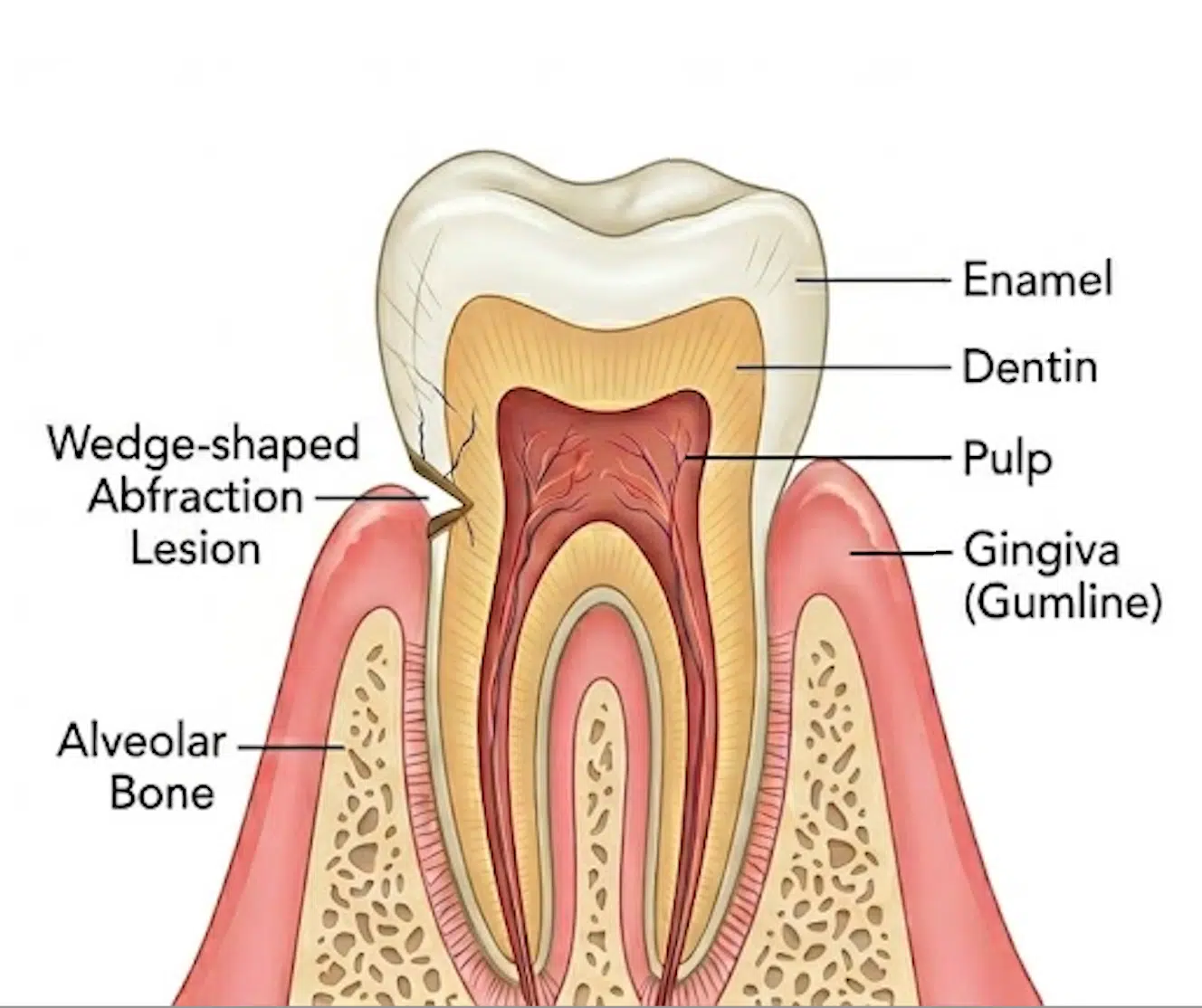
Teeth are not perfectly rigid structures. Under repeated load, they flex—especially near the gumline, where enamel is naturally thinner.
Over time, this flexing concentrates stress at that vulnerable area. Eventually, microscopic breakdown occurs in the enamel structure, leading to the wedge-shaped defects we recognize as abfractions.
Decades ago, an anthropological study examined ancient skulls—long before toothbrushes existed. Researchers observed similar cervical lesions in individuals who clearly never brushed their teeth.
What they did have, however, were signs of heavy occlusal wear and, in many cases, malocclusion.
Even then, the implication was clear: something other than brushing was at work.
Early theories explored mechanisms like piezoelectric effects in enamel. While those ideas have evolved, the core observation still holds—mechanical stress plays a central role.
Why Hard Toothbrushes Still Aren’t Recommended
So if toothbrush abrasion isn’t the main cause of these notches, does that mean brush choice doesn’t matter?
Not at all.
Hard toothbrushes can still damage your teeth and gums—just in a different way.
One important and often overlooked factor is how the bristles are finished.
Soft bristles are typically end-rounded, meaning the tips are polished to be smooth and gentle.
Hard bristles are often cut more bluntly or at angles, leaving sharper edges.
What they generally don’t do is create the deep, wedge-shaped notches associated with abfractions.
Why This Misconception Still Persists
The confusion is understandable.
The location fits the story—damage near the gumline must be from brushing, right?
But dentistry often requires us to look beyond what seems obvious. The mouth is a dynamic system, and forces generated during function (and dysfunction) can have effects that aren’t immediately intuitive.
Clenching, grinding, and bite imbalance can quietly shape tooth structure over years—often without the patient realizing it.
What This Means for You
If you notice notches forming near your gumline, it’s worth looking beyond your brushing habits.
Clenching or grinding habits (especially at night)
Bite alignment and occlusal forces
Stress-related muscle tension
In many cases, addressing those underlying forces is the key to preventing further damage.
Final Thoughts on Toothbrush Abrasion
Toothbrush abrasion is real—but it’s often been blamed for something it doesn’t primarily cause.
The notches we see at the gumline are more accurately a story of stress, flexure, and time.
Understanding that shift doesn’t just correct a misconception—it opens the door to better prevention, more accurate diagnosis, and ultimately, healthier teeth.
Frequently Asked Questions About Toothbrush Abrasion and Gumline Notches
Can brushing too hard cause gumline notches?
It’s a common belief, but brushing too hard is not the primary cause of the wedge-shaped notches seen at the gumline. While toothbrush abrasion can wear down tooth surfaces and irritate gums, these deeper notches are more strongly linked to stress from clenching and grinding.
What is the difference between abrasion and abfraction?
Abrasion refers to mechanical wear caused by external factors like brushing. Abfraction, on the other hand, is thought to result from internal stress forces that cause the tooth to flex, leading to breakdown at the gumline. They can look similar but have very different underlying causes.
Should I stop worrying about toothbrush abrasion?
Not entirely. Toothbrush abrasion can still affect the surface of your teeth and contribute to gum irritation or recession. Using a soft-bristled toothbrush and gentle technique remains important for long-term oral health.
Why do dentists recommend soft toothbrushes?
Soft toothbrushes are designed with end-rounded bristles, which are smoother and less likely to scratch enamel or irritate gums. Hard bristles are often cut more sharply, which can create micro-scratches and contribute to surface wear over time.
How can I tell if I’m grinding or clenching my teeth?
Common signs include jaw soreness, headaches, worn or flattened teeth, and sometimes sensitivity near the gumline. Many people grind at night without realizing it, so a dental exam is often the best way to identify it.
Can these gumline notches be treated or reversed?
Once the structure is lost, it doesn’t grow back on its own. However, your dentist may recommend bonding or other restorative options if the area becomes sensitive or continues to worsen. Just as important is addressing the underlying cause to prevent progression.
What’s the most important takeaway about toothbrush abrasion?
Toothbrush abrasion is only part of the picture. If you’re seeing notches at the gumline, it’s worth looking beyond brushing habits and considering the role of bite forces and long-term mechanical stress.
Tooth pain but X-ray normal is a surprisingly common situation in dentistry. If you have a tooth that hurts even though the X-ray looks normal, it can feel confusing—and sometimes frustrating. But a normal X-ray does not mean nothing is wrong.
Some dental problems are too small, too early, or too subtle to appear clearly on imaging. That is why dentists rely on more than just X-rays to understand what is happening. If you came here after seeing the reel, this is the deeper explanation: pain in a tooth that looks normal on X-ray is often the first sign of a developing issue.
Some causes of tooth pain begin before they become visible on dental X-rays.
Tooth Pain but X-Ray Normal: Why This Happens
When patients experience tooth pain but X-ray normal, it often reflects the limitations of imaging. X-rays are excellent for detecting many structural changes in teeth and bone, but they do not always capture early inflammation, fine cracks, or bite-related stress.
In many cases, pain is the first signal—long before visible damage develops.
7 Possible Causes of Tooth Pain but X-Ray Normal
1. Small cracks in the tooth
Tiny cracks can cause sharp pain when biting or releasing pressure. These are often too fine to show on standard X-rays. This is one reason a cracked tooth can be easy to miss early on. For general background, see the American Association of Endodontists on cracked teeth.
2. Periodontal ligament inflammation
The ligament supporting the tooth can become inflamed from clenching, grinding, or bite imbalance. This can create soreness even when the X-ray appears normal.
3. Early nerve irritation
The pulp inside the tooth may be irritated before any visible damage appears. Sensitivity to temperature or lingering discomfort are common early signs—even when imaging looks unremarkable.
4. Bite imbalance or occlusal stress
Even a slight imbalance in your bite can overload a single tooth, leading to tenderness that does not yet show radiographically. This is especially relevant in people who clench or grind. You may also want to read our related article on bruxism causes.
5. Referred pain
Sometimes the source of pain is not the tooth itself. Sinus pressure, muscle tension, or nearby teeth can all create symptoms that feel like tooth pain—even when the X-ray looks normal.
6. Early decay or leaking restorations
Very small areas of decay or breakdown around fillings may not be visible yet, but can still irritate the tooth.
7. A problem still developing
Some conditions simply have not progressed enough to appear on imaging. This is another reason follow-up matters when symptoms persist.
Why Dentists Do Not Rely on X-Rays Alone
When evaluating tooth pain but X-ray normal, dentists consider far more than imaging. A proper diagnosis may include:
If you have a tooth that hurts despite a normal X-ray, do not ignore it—especially if symptoms persist or worsen.
pain when biting or releasing pressure
lingering sensitivity
pain that wakes you at night
a tooth that feels “off”
These are early warning signs worth evaluating. If clenching or grinding may be part of the picture, our article on bruxism treatment options may also be helpful.
The Bottom Line
Tooth pain but X-ray normal does not mean nothing is wrong. In many cases, it means the problem is subtle, early, or not yet visible on imaging.
If you have a tooth that hurts even though the X-ray looks normal, your symptoms still matter. Early evaluation is often the key to preventing a more significant problem later.
Dr. Richard Walicki is a dentist practicing general and cosmetic dentistry. While we hope you find the information contained herein interesting and useful, this blog is for informational purposes and is not intended to diagnose any oral disease. Dental conditions should be evaluated by your dental health professional or a qualified specialist.
Search by Topic
Get Access To The AWESOME Health Course
In this 12 week program, you’re going to discover how to achieve AWESOME health and double your energy with natural, tested, and scientific strategies. Just click on the image below: